Live broadcasts on Instagram every Sunday at 12:00
Subscribe so you don’t miss out! Subscribe
- home
- Gynecology
- Cervical cancer
- Surgery to remove cervical cancer
Video from the operating room. Laparoscopic surgery for cervical cancer
Over the past decades, cervical cancer has firmly held the second place among cancer diseases in women. The disease is more often diagnosed in women 45-50 years old, but in recent years younger women have been seeking medical help. The only effective treatment for cervical cancer is surgery. However, the choice of technique and scope of intervention is influenced by the stage of the disease, the woman’s age and health, as well as her desire to have a child in the future.
For patients of reproductive age with intraepithelial cancer, conization of the cervix is recommended, and the procedure, performed with one rotation of the conizer, should be sufficiently high and wide. If all pathologically altered tissue is removed, including 1 cm of healthy tissue and ¾ of the endocervix, then the operation can be considered radical.
For pre-invasive or micro-invasive cervical cancer, when the tumor is diagnosed only microscopically, the cervix is removed. This gentle operation can be performed using a scalpel, laser radiation or an electroconizer. In women in menopause, as well as those who have entered the premenopausal period, a total hysterectomy is indicated. If there are contraindications to surgery for cervical cancer, intracavitary radiation therapy is prescribed.
For an invasive tumor, if the depth of invasion does not exceed 5 mm, a total hysterectomy is prescribed. In patients of reproductive age, appendages can be preserved during surgery. Depending on the extent of the tumor cells, removal of part of the vagina, ovaries, and lymphadenectomy may be indicated.
For tumors whose dimensions exceed 5 mm in depth and 7 mm horizontally, an extended hysterectomy is indicated, known as the Wertheim operation, which is an extended intervention including panhysterectomy, removal of the upper third of the vagina, pericervical and peri-vaginal tissue, as well as uterine ligaments and regional lymph nodes , since the determining factor in the prognosis for a malignant process in the cervix is the spread of metastases to regional lymph nodes and other organs. For greater treatment effectiveness, it is possible to prescribe radiation therapy at the stage of preparation for surgery or in the postoperative period.
To determine the stage of the disease in cervical cancer and the extent of damage to neighboring organs, as well as to select the correct surgical treatment tactics, you can send me a description of the ultrasound of the pelvic and abdominal organs, MRI data of the pelvis with contrast, the results of hysteroscopy and histology, to my personal email address, indicate age and main complaints. Then I will be able to give a more accurate answer to your situation.
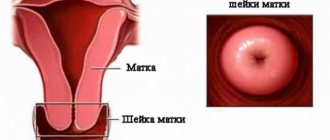
What is cervical cancer?
Worldwide cervical cancer
is the fourth most common cause of death from cancer in women. In 2021, there were 615,000 cases of cervical cancer and 270,000 deaths. This is about 8% of total cancer deaths. In countries with a low level of medicine, a malignant tumor of the cervix is one of the most common causes of death from cancer.
Cervical cancer develops from precancerous changes over 10-20 years. About 90% of cases are squamous cell carcinoma, 10% are cervical carcinoma and a small number of other types. Human papillomavirus (HPV)
causes more than 90% of cases. Most people who have had HPV infections. Other risk factors:
- smoking; weak immune system; onset of sexual activity at an early age;
- birth control pills; having multiple sexual partners; artificial termination of pregnancy.
Stages of cervical cancer
Stage 0: This stage is not truly invasive cancer. The abnormal cells are found only on the surface of the cervix. This stage is called carcinoma in situ (CIS). Stage I: A tumor that has not spread to any lymph nodes, organs, or distant areas of the body. Stage II: The tumor has spread beyond the cervix and uterus, but has not penetrated the pelvic wall or lower part of the vagina. Stage III: The cancer has grown to the lower part of the vagina or pelvic wall. The tumor may block the ureters (tubes that carry urine from the kidneys to the bladder). Stage IV. This is the most advanced stage of cervical cancer. The tumor has spread to the bladder or rectum or to areas in other areas of the body.
At stage 1 of cervical cancer, no symptoms are observed. Later signs include abnormal vaginal bleeding, pain in the pelvis and pain during intercourse. Early diagnosis of cervical cancer is the key to successful treatment of the disease. Oncological screening
using a Pap test allows you to detect precancerous changes. Timely treatment of these pathologies prevents the development of cancer.
Causes and symptoms
Uterine cancer can be either hormone-dependent or autonomous. In the hormone-dependent variant, the endometrium grows due to excessive production of estrogen with low levels of progesterone.
Hyperestrogenism is observed in diabetes mellitus, hypertension, obesity, liver pathologies, taking HRT, and tumors. Clinically, hyperestrogenism is manifested by the following symptoms:
- cycle disruption;
- hyperplasia in the ovarian region;
- infertility;
- late menopause.
The autonomous variant of cancer is less common. As a rule, the disease is typical for older women with low body weight. According to observations, autonomous cancer has a less favorable prognosis.
Cancer development factors:
- heredity;
- obesity;
- diabetes;
- hypertension;
- late onset of menopause;
- absence of pregnancy and childbirth;
- tumors in the ovaries;
- use of Tamoxifen;
- the effect of pelvic irradiation;
- liver diseases.
Cancer of the uterine body in the early stages has no symptoms. As a rule, the first signs appear in the second or third stage. Manifestations of cancer include:
- uterine bleeding;
- increase in the amount of menstrual flow;
- leucorrhoea;
- purulent, bloody, watery discharge;
- pain syndrome;
- disorders associated with the functioning of the bladder, intestines and kidneys;
- swelling;
- deterioration in general health;
- noticeable weight loss.
An alarming sign is bloody discharge in women after menopause in any quantity.
How to treat cervical cancer?
Treatment for cervical cancer depends on the stage of the disease and the severity of the pathology. There are four main treatment options: surgery, radiation therapy, chemotherapy and targeted therapy. A combination of them is possible.
Surgery
The goal of the surgery is to remove as much cancer as possible. Sometimes the doctor can remove only the area of the cervix that contains cancer cells. For later stages of the disease, removal of the cervix and other pelvic organs is indicated.
Radiation therapy
Radiation kills cancer cells using high-energy X-rays. It is used at different stages of the disease. Effective at the initial stage of cervical tumor development.
Chemotherapy
Chemotherapy uses drugs to kill cancer cells throughout the body. To achieve maximum effect, the patient receives chemical drugs in courses. This allows you to destroy cancer cells without harming the body.
Targeted therapy
Targeted drugs block the growth of new blood vessels that help feed the tumor. They target cancer cells and do not damage healthy tissue. Often targeted drugs are prescribed along with chemotherapy.
Preliminary tests and examinations
Before surgery, the patient undergoes the following examinations:
- gynecological examination and colposcopy;
- collection of smears for microscopic examination of microflora;
- general and detailed blood test;
- research on tumor markers;
- ultrasound examination of the pelvic organs;
- computed tomography and magnetic resonance imaging to clarify the localization and extent of the oncological process;
- biopsy - in most cases, the final diagnosis is made after conization during histological analysis of the removed tissue.
Main indications for surgery for cervical cancer
The decision on possible surgical removal of a cervical tumor is made by the doctor after a thorough diagnosis and determination of the stage of the disease. The main indication for surgery for cervical cancer
is an early stage of development of the oncological process. Surgical treatment (including in combination with other methods of therapy) is most often possible at stage IA1, stages IA2, IB1, IB1 (if the tumor is operable), as well as at stage IIA (if the size of the tumor does not exceed 4 cm). The degree of radicality of the operation depends on the characteristics of the oncological process, as well as the need to preserve reproductive function.
Operation
Her method depends on the health and age of the patient, the degree of spread of the malignant process. Spinal anesthesia (an anesthetic is injected into the spinal canal) or anesthesia with controlled breathing is used. The volume is planned at the stage of its preparation, but may change during its implementation after examination of the abdominal organs.
Types of hysterectomy:
- subtotal - supravaginal amputation of the uterus with preservation of the cervix;
- total - removal of the body, cervix.
In most cases, after surgery, a treatment method such as radiotherapy is prescribed to prevent relapses.
Types of surgeries for cervical cancer
For in situ cervical cancer, surgery is performed using minimally invasive methods, as well as using laser and cryosurgery methods. At stage 0 of squamous cell carcinoma of the cervix, surgery can be performed on an outpatient basis, with local anesthesia and within one visit to a specialist. This type of procedure includes loop electroexcision of the cervix and cryoconization.
Laser conization requires general anesthesia, but is also a low-traumatic procedure and does not have a long list of negative postoperative consequences.
For microinvasive cervical cancer, organ-preserving operations are also used, which are performed using laparoscopic and robotic surgery.
In the case of cervical adenocarcinoma of stages 0 and 1, resection of the tissue affected by the tumor process is performed - conization of the cervix - an operation that involves preserving the opportunity to have children.
At stage 1 of cervical cancer, an operation to completely remove the organ - a total hysterectomy (in addition to the uterus itself, its appendages are removed) may be indicated. After surgery for stage 1 cervical cancer, radiotherapy and/or chemotherapy may be prescribed to prevent future recurrence. Surgery for stage 2 cervical cancer also involves complete resection of the uterus and appendages, as well as para-aortic and pelvic lymph nodes.
- The gold standard of surgery for cervical cancer is the Wertheim procedure. This method, in various improved versions, is used by surgeons around the world. Wertheim's operation for cervical cancer consists of resection of the uterus with appendages, the upper third of the vagina, peri-uterine tissues and regional (closest) lymph nodes. The method involves removing adjacent healthy tissue, which minimizes the possibility of relapse.
- For stage 3 cervical cancer, surgery is performed extremely rarely. As a rule, radiotherapy and chemotherapy methods are used. However, at stage 3A, when the malignant neoplasm is localized within the pelvis and upper third of the vagina, an experienced surgeon can perform radical surgery. The ability to perform surgery in combination with other methods of therapy increases the chances of recovery at stage 3A to 60%.
Types and methods of hysterectomy
Depending on the volume of the operation, the following types are distinguished:
- Subtotal, or amputation - removal of the uterus without or with appendages, but preserving the cervix.
- Total, or hysterectomy, is the removal of the body and cervix with or without appendages.
- Panhysterectomy - removal of the uterus and ovaries with fallopian tubes.
- Radical - panhysterectomy in combination with resection of the upper 1/3 of the vagina, with removal of part of the omentum, as well as the surrounding pelvic tissue and regional lymph nodes.
Currently, abdominal surgery to remove the uterus is carried out, depending on the access option, in the following ways:
- abdominal, or laparotomy (a midline incision in the tissues of the anterior abdominal wall from the umbilical to the suprapubic region or a transverse incision above the pubis);
- vaginal (removal of the uterus through the vagina);
- laparoscopic (through punctures);
- combined.
Laparotomy (a) and laparoscopic (b) access options for hysterectomy surgery
Abdominal access method
It has been used most often and for a very long time. It is about 65% when performing operations of this type, in Sweden - 95%, in the USA - 70%, in the UK - 95%. The main advantage of the method is the possibility of performing surgical intervention under any conditions - both during planned and in case of emergency surgery, as well as in the presence of other (extragenital) pathology.
At the same time, the laparotomy method also has a large number of disadvantages. The main ones are the serious traumatic nature of the operation itself, a long hospital stay after the operation (up to 1–2 weeks), prolonged rehabilitation and unsatisfactory cosmetic consequences.
The postoperative period, both immediate and long-term, is also characterized by a high incidence of complications:
- long-term physical and psychological recovery after hysterectomy;
- adhesive disease develops more often;
- it takes a long time for intestinal function to be restored and the lower abdomen hurts;
- high, compared to other types of access, the likelihood of infection and increased temperature;
Mortality with laparotomy access per 10,000 operations averages 6.7-8.6 people.
Vaginal removal
It is another traditional access used for hysterectomy. It is carried out through a small radial dissection of the vaginal mucosa in its upper parts (at the level of the fornix) - posterior and possibly anterior colpotomy.
The undeniable advantages of this access are:
- significantly less trauma and the number of complications during surgery compared to the abdominal method;
- minimal blood loss;
- short duration of pain and better health after surgery;
- rapid activation of the woman and rapid restoration of intestinal function;
- short period of hospital stay (3-5 days);
- good cosmetic result, due to the absence of an incision in the skin of the anterior abdominal wall, which allows the woman to hide the very fact of surgical intervention from her partner.
The recovery period with the vaginal method is much shorter. In addition, the frequency of complications in the immediate postoperative period is low and there are no complications in the late postoperative period, and mortality is on average 3 times less than with abdominal access.
At the same time, vaginal hysterectomy also has a number of significant disadvantages:
- the lack of a sufficient area of the surgical field for visual inspection of the abdominal cavity and manipulation, which significantly complicates the complete removal of the uterus for endometriosis and cancer, due to the technical difficulty of detecting endometriotic foci and tumor boundaries;
- high risk of intraoperative complications in terms of injury to blood vessels, bladder and rectum;
- difficulties in stopping bleeding;
- the presence of relative contraindications, which include, in addition to endometriosis and cancer, significant tumor sizes and previous operations on the abdominal organs, especially on the lower organs, which can lead to changes in the anatomical location of the pelvic organs;
- technical difficulties associated with uterine retraction in obesity, adhesions and in nulliparous women.
Due to such restrictions, in Russia vaginal access is used mainly for operations for prolapse or prolapse of an organ, as well as for gender reassignment.
Laparoscopic access
In recent years, it has become increasingly popular for any gynecological operations in the pelvis, including hysterectomy. Its benefits are largely identical to the vaginal approach. These include a low degree of trauma with a satisfactory cosmetic effect, the possibility of cutting adhesions under visual control, a short recovery period in the hospital (no more than 5 days), a low incidence of complications in the immediate and their absence in the long-term postoperative period.
However, there are still risks of such intraoperative complications as the possibility of damage to the ureters and bladder, blood vessels and large intestine. The disadvantage is also the limitations associated with the oncological process and the large size of the tumor formation, as well as with extragenital pathology in the form of even compensated cardiac and respiratory failure.
How is the operation for cervical cancer performed and how many hours does it last?
Abdominal surgery is performed through a fairly large incision in the abdominal cavity. An open hysterectomy lasts from 40 minutes to 2 hours.
Laparoscopic surgery is considered less traumatic. To do this, before the manipulations begin, the abdominal cavity is filled with gas in order to raise the abdominal wall and open access to the uterus.
Next, tubes are inserted through small incisions. They create a path for the insertion of instruments and the camera. This operation lasts 1.5-3.5 hours.
In the best clinics in the world, hysterectomy is performed using the da Vinci robot. This operation is recognized as the most gentle and most effective, since it ensures high precision in the removal of affected tissue. The Robot's instruments are inserted through minimal incisions, and all its movements are controlled by the surgeon, who sees the surgical field in 3D and multiple magnification. This method preserves sexual function for patients and ensures little blood loss, and the operation itself lasts only 1 hour.
Preparing for surgery for cervical cancer
Before the operation, you are prescribed to undergo a series of examinations. Based on the results of diagnosis and communication with the patient, the final decision on the type of operation is made. However, before surgery, you must agree to a more radical intervention if absolutely necessary. The patient can choose the type of anesthesia: general anesthesia or epidural anesthesia (local anesthesia by injecting a drug into the epidural space of the spine).
The day before surgery, a woman should switch to light food. Some doctors also prescribe sedatives. Before the operation, you need to take a shower, remove hair from the pubic area, refuse food and liquid (6-8 hours before), cleanse the intestines (give an enema). The operation is prescribed for the period from the end of menstruation to the onset of ovulation.
What you should pay attention to during the rehabilitation period
Those women who have undergone treatment for uterine cancer experience various changes in the body, which, in turn, require special rehabilitation measures. Let's look at what both the doctor and the patient should pay attention to.
Psychological condition.
As a rule, many women are emotionally tense, anxious, stressed and afraid. At the stage of diagnosis and treatment, it is worth surrounding the patient with attention, care, and creating a favorable environment. If possible, doctors need to talk to the woman during the first conversation that depression, withdrawal and other negative thoughts are not a solution to the problem, that first they should get accurate examination data, and then act according to the situation. During treatment, the specialist may recommend taking certain medications to reduce anxiety or use other methods to correct the psychological state.
Inhibition of hematopoiesis, trophic damage to the intestines and bladder.
During the rehabilitation period, you should eat food that is rich in proteins, fats and microelements, namely, contains the required amount. Various conditions associated with trophic damage to the bladder are corrected by a doctor with the help of medications.
Cervical cancer: how long do they live after surgery?
- The prognosis after surgery for cervical cancer
is quite comforting. Surgery and its combination with other methods provide a high chance of survival. To minimize the occurrence of relapse after surgery for cervical cancer, radiation therapy and/or chemotherapy are performed. Survival rates after surgery for stage 1 and 2A cervical cancer reach 88-99% (if the lymph nodes are not affected). If lymph nodes are affected, the prognosis for treatment at stages 1 and 2 is reduced to 50-74%.
Cost of surgery for cervical cancer
The cost of surgical treatment of cervical cancer depends on the severity of the disease, stage and methods used to treat oncopathology. The cost is also affected by the level of the clinic and the qualifications of the doctor. The lowest prices for surgery for cervical cancer are observed in Turkey and South Korea. Treatment in Spain, Germany, Israel and Austria will cost 20-40% more. For more information on prices for cervical cancer surgeries in other countries, please follow the link.
Reviews about surgery for cervical cancer
Where it was held:
Ichilov Clinic
What procedure:
Surgery for cervical cancer
Patient age:
47 years old
Patient from:
Kiev
Anna:
“In 2021, we learned that my aunt had cervical cancer. They refused to perform the operation at the local hospital. They put the 3rd suspicion at stage 4 and offered palliative treatment. We did not accept this fact and decided to go to Israel for additional diagnostics. There they determined stage 3A. The diagnosis took place at the Assuta clinic, and at the Ikhilov clinic they found a doctor who began to operate. A radical hysterectomy was performed, operated by Prof. Dan Grisaro. Now the disease has subsided, my aunt feels well. We are very glad that we did not resign ourselves then, but decided to fight, and turned to real professionals who helped us with this...”
To arrange a trip to surgery to remove cervical cancer, please contact the coordinating doctors of the international medical platform MediGlobus. Our specialists will answer all your questions and select the best treatment option for you.
Rating: 5
Oncology
Doctor Vadim Berezhnoy
General practitioner, Medical expert, Head of the department of doctors-coordinators.
Albina Golovina
Works in the field of medical copywriting for 2 years. She is a postgraduate student at the Faculty of Psychology. Author of several scientific publications in the field of clinical psychology. Additionally he studies the physiology of the central nervous system, neuropsychology and psychiatry. In her spare time, she studies mindfulness practices and conducts psychological consultations.
Postoperative consequences
The most severe postoperative consequences of uterine cancer are the complete removal of a woman’s reproductive organs. The fourth stage of uterine cancer is characterized by damage not only to the internal genital organs, but also to the surrounding vital organs of the urinary system and intestines. In such a situation, we are no longer talking about saving the woman’s reproductive function, there is a fight for the patient’s life, so they are trying to save vital organs.
The situation is a little better when doctors manage to save the vagina and ovaries. In this case, the hormonal background of the body does not change significantly, the woman, of course, cannot have children, but the positive thing is that hormone replacement therapy is not required and after recovery, you can lead a normal life.
The situation is worse when you have to undergo an oophorectomy (removal of the ovaries), because the woman not only loses her reproductive function, but is also forced to regularly take hormonal medications to maintain normal hormonal balance in the body.
When uterine cancer is detected at an early stage and treated in a timely manner, the reproductive organs are almost always completely preserved. However, here, too, various complications and side effects are possible. A surgical operation, especially of the abdominal type, causes injury to the tissues of the body, therefore the main complications after such operations are adhesions and various compactions of the uterus. Another disadvantage is the long rehabilitation period.
Among other things, one should take into account such factors as chemotherapy and radiation therapy, which, in the vast majority of cases, accompany operations to remove tumors, both before and after them. And in order to recover from such therapy, the body requires at least three years.