A functional ovarian cyst is a hollow, thin-walled formation growing from the ovarian tissue, filled with fluid inside. Functional cysts are benign. Most often diagnosed in women of reproductive age. Approximately 10-15% of tumor-like formations in postmenopausal women are prone to malignancy. Any neoplasm is considered to be a cyst if its size exceeds 2.5-3 cm in diameter.
The Yusupov Hospital offers a huge selection of medical and surgical treatments for functional ovarian cysts. Within the hospital, the patient undergoes a full clinical and laboratory examination using high-tech diagnostic equipment. After receiving the results of functional tests, the gynecologist draws up an individual treatment plan for each patient. Despite the narrow profile of the disease, the clinic’s specialists adhere to an integrated approach to therapy, so the patient is also advised by related doctors: endocrinologist, cardiologist, neurologist. The Yusupov Hospital is proud not only of its modern equipment, but also of its professional medical staff, ready to help at any time.
Functional ovarian cyst: types
Functional ovarian cysts are formed as a result of natural physiological processes in a woman’s body. Therefore, despite the fact that this group of cystic pathologies is classified as tumor-like formations, they are not tumors as such. Depending on the source of occurrence, the following types of functional cysts are distinguished:
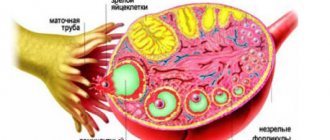
- Follicular cysts - develop from a dominant follicle in the absence of ovulation. In gynecology, they make up about 80% of all ovarian cysts. Upon closer examination, the follicular cyst has the appearance of a round single-chamber formation, with clear contours and smooth walls, filled with dark yellow liquid content. Over time, these cysts regress on their own, only in rare cases they are capable of malignancy;
- Corpus luteum cyst or luteal cyst is formed against the background of a non-regressed corpus luteum. As a result of impaired blood circulation and lymph outflow, fluid begins to accumulate in the ovarian tissues, which in the future will fill the entire cavity of the ovarian corpus luteum cyst.
Taking into account the theory of genetic determination, which tells us about earlier and highly functional activity of the right ovary, it should be clarified that cystic formations of the female reproductive genital organs can only be unilateral. Ultrasound reveals either a functional cyst of the left ovary or a functional cyst of the right ovary.
Rational attitude to the diagnosis of polycystic ovary syndrome
The diagnosis of polycystic ovary syndrome (PCOS) is the subject of many misconceptions. We offer a practically oriented consideration of this problem and its associated uncertainties.
In the minds of many people, the diagnosis of polycystic ovary syndrome (PCOS) is associated with a very specific idea of an “endocrine disease”.
In many sources, definitive information about PCOS is accompanied by images or photographs of altered ovaries that have nothing to do with this syndrome and form a distorted idea of the structure of the ovaries in PCOS.
This understanding is very superficial and gives rise to a number of serious consequences, including, but not limited to, overuse of diagnostic services, overtreatment, unnecessary stress, distraction from truly important issues, and neglect of valuable opportunities for self-care.
The condition of women of reproductive age who have at least 2 of the following 3 signs:
— Excessive activity of male sex hormones (androgens), which is manifested by an increase in the level of androgens in the blood and/or excessive hair growth on the face or in various androgen-dependent areas of the body;
- Ovulation disorder, which may manifest itself with symptoms such as irregular menstruation and/or difficulty conceiving a child;
— Changes in the structure of the ovaries, ascertained by ultrasound.
According to the updated definition, signs of PCOS are the presence of more than 25 follicles in the ovary with a diameter of 2 to 9 mm and/or an ovarian volume greater than 10 ml. And in whom, after adequate examination, other causes of the listed symptoms were excluded.
To form a practically oriented understanding of the diagnosis of PCOS, it is necessary to consider in parallel the different components of this definition.
PCOS can present differently in different women.
66% of women with this diagnosis have all three signs, that is:
- increased activity of male sex hormones (increased testosterone levels in the blood and/or excess hair growth or, to a lesser extent, acne),
- ovulation disorders and
- a characteristic change in the structure of the ovaries.
In 13% of women, PCOS manifests:
— increased activity of male sex hormones (increased testosterone levels in the blood and/or excess hair growth) and
- changes in ultrasound structure of the ovaries, but without signs of impaired ovulation.
In 11% of women, polycystic ovary syndrome manifests itself:
- ovulation disorders,
- changes in the structure of the ovaries, but without signs of increased activity of male sex hormones.
In 9% of women, PCOS manifests itself:
— increased activity of male sex hormones (increased testosterone levels in the blood and/or excess hair growth on the face or body), and
— ovulation disturbance, but without a characteristic change in the structure of the ovaries .
There are several more rare forms (phenotypes) of this disorder, formed from different combinations of the listed symptoms.
This means that the diagnosis of PCOS does not refer to any specific disease, but to a group of relatively poorly understood conditions with more or less overlapping, but at the same time different manifestations. It is possible that in the future the different phenotypes of PCOS will be considered as separate conditions.
The diagnosis of PCOS can only be made in women of reproductive age
In girls during the first two years after the onset of menstruation and in women approaching menopause, a diagnosis of PCOS is impossible, since ovulation disorders and irregular menstruation are a physiological phenomenon during these periods of life.
In addition, for adolescents, the presence of numerous follicles in the ovaries is a normal phenomenon, and standards for assessing androgen levels for adolescent girls have not been established.
Pimples (acne) are present in most adolescents and at this age cannot be considered a sign of excessive androgen activity.
Excessive hair growth on the face or body, characteristic of PCOS, develops slowly and may not become noticeable until several years after the onset of puberty.
The manifestations and natural progression of PCOS in women who have reached menopause are unknown.
A change in the structure of the ovaries, noticeable on ultrasound, is one of the possible, but not mandatory criteria for diagnosing PCOS
Some women diagnosed with PCOS have ovaries with the same structure as women without PCOS.
If a woman already has symptoms of ovulation disorders and symptoms of androgen excess (increased testosterone levels, excess hair growth), an ovarian ultrasound is not necessary to confirm the diagnosis of PCOS.
In recent years, the diagnostic criteria for PCOS have undergone significant changes. Until 2003, an ultrasound sign of PCOS was considered to be the presence in the ovary of more than 12 follicles with a diameter of 2 to 9 mm and/or a total ovarian volume of more than 10 ml. After a number of studies showed that the ovaries of most women have the same or similar structure, at the suggestion of a number of experts, an updated definition was drawn up: a sign of PCOS is the presence in the ovary of more than 25 follicles with a diameter of 2 to 9 mm and/ or ovarian volume is more than 10 ml.
PCOS is a diagnosis of exclusion
The expression “diagnosis of exclusion” means that the diagnosis of PCOS can only be made after all other causes/diseases that may cause similar symptoms have been excluded.
There are several important conclusions associated with this:
(A) Diagnosing PCOS is only valuable if a woman has obvious symptoms.
(B) Making a diagnosis of PCOS and ruling out other diseases is only necessary to determine whether a woman can gain any value from specific medical intervention or additional counseling.
(B) There is no standard algorithm for diagnosing PCOS. Diagnostic tactics depend on what symptoms bother the woman.
Before starting a diagnosis, a woman and her healthcare provider should carefully discuss the limitations and actual usefulness of different diagnostic tests to avoid wasting resources and time on unnecessary tests.
Depending on the symptoms, a woman can choose one of the following diagnostic algorithms:
(1) Diagnostic algorithm for irregular menstruation
(2) Diagnostic algorithm for difficulties conceiving a child
(3) Diagnostic algorithm for excessive hair growth.
PCOS is a "disorder" only in a statistical sense
As with many other conditions, when discussing the meaning of a diagnosis of polycystic ovary syndrome, the physician and patient need to take special care to consider the basis on which a condition is considered a “disease” or “disorder.”
You should think of PCOS only as a disorder in a statistical sense. It is only called a "disease" because most women do not have the symptoms and appearances that some women with this condition have.
It is true that women with PCOS are more likely to experience certain “health problems,” but tying attributes such as “excess hair growth” or “irregular periods” to the category of “symptoms” means that we evaluate these phenomena through the lens of social norms and statistics rather than strictly pathophysiological criteria.
When talking about the diagnosis of PCOS, one should not neglect important information about the real level of short-term and long-term risks
Information about the risks associated with a diagnosis of polycystic ovary syndrome is often presented in a grossly unbalanced manner, without context or comparison. It can be assumed that in many women such information causes a significantly exaggerated idea of the danger of the disease.
Infertility is often mentioned as one of the possible consequences of PCOS, although on average, women with the condition have almost the same chance of conceiving and carrying a child to term as women without PCOS. It is true that women with polycystic ovary syndrome are more likely than other women to experience ovulation problems, but in most cases a couple can overcome this problem by trying a little longer to conceive.
In addition, it is a mistake to imagine infertility with PCOS as some kind of progressive problem that will increase if a woman does not take treatment.
High blood pressure and diabetes are often described as other consequences of PCOS. It is true that women with this diagnosis experience these health problems somewhat more often than other women, but you need to understand that many people develop high blood pressure in one way or another. At different periods of life, diabetes mellitus is diagnosed in almost 40% of adults. High blood pressure and diabetes are not problems specific to women with PCOS. Additionally, having this diagnosis does not mean that a woman will necessarily have these health problems. As with many other diseases, many factors are involved in the development of diabetes and high blood pressure, and the presence of PCOS is only one of them.
Increased risk of cancer. This is probably the most frightening complication of PCOS, but one must remain rational in this regard. Some women with PCOS do have a higher risk of developing endometrial cancer, but this only applies to women with significantly irregular menstrual cycles. In addition, it should be emphasized that in these women, the risk of developing cancer can be very well controlled by hormonal contraceptives, and that in adulthood and as people approach menopause, the likelihood of developing endometrial cancer increases in all women, not just women with PCOS.
Conclusion: what does the diagnosis of “polycystic ovary syndrome” mean and what is the value of diagnosing this condition?
From the above, several important conclusions can be drawn:
(1) A diagnosis of PCOS means that a woman has certain characteristics of the functioning of the endocrine system that are not characteristic of most other women from her ethnic group.
(2) The only reason a PCOS diagnosis is valuable to a woman is because it allows her to understand whether she can get any value from making any specific changes to her self-care plan.
(3) Diagnosis of PCOS should always be made only in the context of the symptoms that are bothering the woman. In this regard, getting a diagnosis helps you choose the most appropriate treatment options to relieve your symptoms and take care of yourself.
For complete recommendations regarding PCOS, see: Self-Care Plan for Women with Polycystic Ovarian Syndrome
Author: Alexander Kasapchuk.
Sources:
- Azziz, Ricardo, Enrico Carmina, Didier Dewailly, Evanthia Diamanti-Kandarakis, Héctor F. Escobar-Morreale, Walter Futterweit, Onno E. Janssen, et al. “The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report.” Fertility and Sterility 91, no. 2 (2009): 456-488. doi:10.1016/j.fertnstert.2008.06.035.
- Bachanek, Michał, Nebil Abdalla, Krzysztof Cendrowski, and Włodzimierz Sawicki. “Value of ultrasonography in the diagnosis of polycystic ovary syndrome – literature review.” Journal of Ultrasonography 15, no. 63 (2015): 410-422. doi:10.15557/jou.2015.0038.
- Conway, G., D. Dewailly, E. Diamanti-Kandarakis, H. F. Escobar-Morreale, S. Franks, A. Gambineri, F. Kelestimur, et al. “The polycystic ovary syndrome: a position statement from the European Society of Endocrinology.” European Journal of Endocrinology 171, no. 4 (2014): P1-P29. doi:10.1530/eje-14-0253.
- Dewailly, D., M. E. Lujan, E. Carmina, M. I. Cedars, J. Laven, R. J. Norman, and H. F. Escobar-Morreale. “Definition and significance of polycystic ovarian morphology: a task force report from the Androgen Excess and Polycystic Ovarian Syndrome Society.” Human Reproduction Update 20, no. 3 (2013): 334-352. doi:10.1093/humupd/dmt061.
- Fauser, Bart C., Basil C. Tarlatzis, Robert W. Rebar, Richard S. Legro, Adam H. Balen, Roger Lobo, Enrico Carmina, et al. “Consensus on women's health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group.” Fertility and Sterility97, no. 1 (2012): 28-38. doi:10.1016/j.fertnstert.2011.09.024.
- Goodman, Neil F., Rhoda H. Cobin, Walter Futterweit, Jennifer S. Glueck, Richard S. Legro, and Enrico Carmina. “American Association Of Clinical Endocrinologists, American College Of Endocrinology, And Androgen Excess And PCOS Society Disease State Clinical Review: Guide To The Best Practices In The Evaluation And Treatment Of Polycystic Ovary Syndrome – Part 1.”Endocrine Practice 21, no. 11 (2015): 1291-1300. doi:10.4158/ep15748.dsc.
- Legro, Richard S., Silva A. Arslanian, David A. Ehrmann, Kathleen M. Hoeger, M. H. Murad, Renato Pasquali, and Corrine K. Welt. “Diagnosis and Treatment of Polycystic Ovary Syndrome: An Endocrine Society Clinical Practice Guideline.” The Journal of Clinical Endocrinology & Metabolism 98, no. 12 (2013): 4565-4592. doi:10.1210/jc.2013-2350.
- Palomba, Stefano, Susanna Santagni, Angela Falbo, and Giovanni B. La Sala. “Complications and challenges associated with polycystic ovary syndrome: current perspectives.”International Journal of Women's Health, no. 7 (2015): 745-763. doi:10.2147/ijwh.s70314.
- “Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome.” Fertility and Sterility 81, no. 1 (January 2004): 19-25. doi:10.1016/j.fertnstert.2003.10.004.
- Rojas, Joselyn, Mervin Chávez, Luis Olivar, Milagros Rojas, Jessenia Morillo, José Mejías, María Calvo, and Valmore Bermúdez. “Polycystic Ovary Syndrome, Insulin Resistance, and Obesity: Navigating the Pathophysiologic Labyrinth.” International Journal of Reproductive Medicine 2014 (2014): 1-17. doi:10.1155/2014/719050.
- Royal College of Obstetricians and Gynecologists. “Long-term Consequences of Polycystic Ovarian Syndrome.” Green-top Guideline No. 33, 2014, 1-15.
- Sirmans, Susan, and Kirsten Pate. “Epidemiology, diagnosis, and management of polycystic ovary syndrome.” Clinical Epidemiology, no. 6 (2014): 1-13. doi:10.2147/clep.s37559.
- Talaei, Afsaneh, Zahra Adgi, and Mahnaz Mohamadi Kelishadi. “Idiopathic Hirsutism and Insulin Resistance.” International Journal of Endocrinology 2013 (2013): 1-5. doi:10.1155/2013/593197.
- Wierman, Margaret E., Wiebke Arlt, Rosemary Basson, Susan R. Davis, Karen K. Miller, Mohammad H. Murad, William Rosner, and Nanette Santoro. “Androgen Therapy in Women: A Reappraisal: An Endocrine Society Clinical Practice Guideline.” The Journal of Clinical Endocrinology & Metabolism99, no. 10 (2014): 3489-3510. doi:10.1210/jc.2014-2260.
- Wild, Robert A., Enrico Carmina, Evanthia Diamanti-Kandarakis, Anuja Dokras, Hector F. Escobar-Morreale, Walter Futterweit, Rogerio Lobo, Robert J. Norman, Evelyn Talbott, and Daniel A. Dumesic. “Assessment of Cardiovascular Risk and Prevention of Cardiovascular Disease in Women with the Polycystic Ovary Syndrome: A Consensus Statement by the Androgen Excess and Polycystic Ovary Syndrome (AE-PCOS) Society.” The Journal of Clinical Endocrinology & Metabolism95, no. 5 (2010): 2038-2049. doi:10.1210/jc.2009-2724.
- Bates, Gordon W., and Joshua Berger. “Optimal management of subfertility in polycystic ovary syndrome.” International Journal of Women's Health, no. 6 (2014): 613-621. doi:10.2147/ijwh.s48527.
- Bouchard, P. “Treatment of infertility in women with polycystic ovary syndrome.” Annales d'Endocrinologie 71, no. 3 (2010): 225-227. doi:10.1016/j.ando.2010.03.006.
- Costello, Michael F., and William L. Ledger. “Evidence-based management of infertility in women with polycystic ovary syndrome using surgery or assisted reproductive technology.” Women's Health 8, no. 3 (2012): 291-300. doi:10.2217/whe.12.7.
- Hueb, Cristina K., João A. Dias Júnior, Maurício S. Abrão, and Elias K. Filho. “Drilling: medical indications and surgical technique.” Revista da Associação Médica Brasileira 61, no. 6 (2015): 530-535. doi:10.1590/1806-9282.61.06.530.
- Melo, A. S., R. A. Ferriani, and P. A. Navarro. “Treatment of infertility in women with polycystic ovary syndrome: approach to clinical practice.” Clinics 70, no. 11 (2015): 765-769. doi:10.6061/clinics/2015(11)09.
- The Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. “Consensus on infertility treatment related to polycystic ovary syndrome.” Fertility and Sterility 89, no. 3 (2008): 505-522. doi:10.1016/j.fertnstert.2007.09.041.
- Vause, Tannys D., Anthony P. Cheung, Sony Sierra, Paul Claman, James Graham, Jo-Anne Guillemin, Louise Lapensée, Sabrina Steward, Tannys D. Vause, and Benjamin C. Wong. “The Society of Obstetricians and Gynecologists of Canada Clinical Practice Guideline: Ovulation Induction in Polycystic Ovary Syndrome.” International Journal of Gynecology & Obstetrics 111, no. 1 (2010): 95-100. doi:10.1016/j.ijgo.2010.07.001.
Functional ovarian cyst: causes
The development of this disease is based on endocrine metabolic disorders that contribute to hormonal imbalance (hyperestrogenemia) and the development of an anovulatory menstrual cycle. If ovulation is disrupted, the dominant follicle continues to increase in size as a result of the accumulation of fluid in it (retention). This is how a follicular cyst is formed. If the corpus luteum does not regress, then a cyst is formed at its base, into the cavity of which hemorrhages can occur.
Risk factors for the development of functional ovarian cysts in women may include:
- Stress, stressful conditions;
- Physical fatigue;
- Hormonal disorders;
- Excess body weight and metabolic syndrome;
- Poor lifestyle, smoking, alcohol;
- Taking glucocorticoids or hormonal contraceptives;
- Chronic inflammatory processes in the pelvic organs;
- Frequent abortions;
- External endometriosis;
- Adhesive process in the pelvis;
- Ovarian resection or unilateral oophorectomy.
Functional cyst of the right and left ovary: what is it and how to treat?
Many women, upon hearing such a diagnosis, panic, believing that this disease is very dangerous. However, cystic formations often resolve on their own. If this does not happen, treatment is prescribed. Complex cases require surgical intervention.
What does a functional ovarian cyst mean?
Sometimes during ovulation, women may feel pain and discomfort in the lower abdomen. In this case, doctors suspect the development of a functional cyst of the left ovary.
The process is associated with malfunctions in the reproductive system, as a result of which the follicle can stretch and fill with fluid if the egg leaves it or remains inside.
This formation resolves on its own after several menstrual cycles. When the process creates discomfort, doctors prescribe treatment.
Follicular ovarian cysts are benign. They develop when the egg does not leave the follicle.
The growth of formation occurs when fluid is released from nearby vessels carrying blood and lymph, or when secretion continues to be produced by granulosa-type epithelial cells. If the cyst is about 5 cm in size, it dissolves on its own, without the help of medications.
Drug intervention requires a neoplasm that continues to grow up to 6 cm. There are cases when drugs do not have an effect and surgery must be performed.
A luteal functional cyst of the left ovary is formed after the release of the egg from the follicle and its transformation into the corpus luteum, which produces the hormones necessary for pregnancy.
When conception does not occur, the endocrine gland disappears on its own after some time, and the cyst disperses along with it. However, there is a possibility that the corpus luteum will fill with fluid, which will then remain on the ovary.
Such a cyst does not show itself with symptoms, and is often detected during routine examinations.
A retention cyst is a benign neoplasm that fills with water or blood. The reasons for its occurrence can be various factors, among which the most common are:
- disruptions in a woman’s endocrine system;
- abortions performed many times, resulting in consequences;
- excessively rapid rate of puberty;
- diseases arising in the endocrine system;
- hypothyroidism
Signs
A retention functional cyst of the left ovary may not manifest itself in any way, however, in some cases, when such a pathology occurs, the following symptoms may form:
- acute pain in the lower abdomen;
- feeling of pressure or heaviness in the pelvic area;
- irregular menstrual cycle;
- prolonged pain during menstruation;
- nausea that occurs after exercise;
- feeling of pressure when defecating or urinating;
- bloody vaginal discharge accompanied by pain.
There are symptoms that are more dangerous to a woman’s health; if they are detected, you should visit a doctor:
- temperature rise of more than 38 degrees;
- hair growth in areas characteristic of men;
- dizziness and general weakness;
- menstruation, characterized by heavy discharge;
- increase in abdominal volume;
- blood pressure readings that deviate from the norm;
- frequent need to drink;
- increased volume of urine when urinating;
- the presence of lumps in the abdominal cavity that can be palpated.
Treatment of a functional cyst of the left ovary
Measures to get rid of cystic tumors come down to 2 options:
- conservative therapy;
- surgical intervention.
How to treat a corpus luteum cyst
If the retention formation does not disappear on its own within several menstrual cycles, it is treated with therapeutic methods, including:
- medicines;
- electrophoresis;
- magnetic therapy;
- ultraphonophoresis;
- laser therapy.
Medicines used for corpus luteum cyst are aimed at eliminating it, improving blood circulation, restoring hormonal balance and combating possible inflammatory processes. The following tablets have proven themselves well in this area:
- Tsvilin;
- Medvitsin;
- Livicin.
In addition, Duphaston can be used: it is a progesterone substitute. The main effect of the drug is aimed at reducing the size of the formation, however, it can be taken in the absence of the following contraindications:
- liver diseases;
- poor blood clotting;
- tumors of a malignant nature.
During the therapy period, the patient must avoid heavy physical activity and should also avoid sex for a while. Failure to comply with these rules may cause twisting of the pedicle of the FJ, which will negatively affect the progress of treatment.
All this time, the woman must be under the supervision of a doctor, who after a couple of months should determine whether the therapy is helping. If the cyst continues to grow, a decision is made about the need for surgical intervention.
If the decision is positive, the patient undergoes laparoscopy. However, if bleeding occurs or the cyst is too large and may burst, the intervention method changes to laparotomy.
These symptoms may indicate the need to completely remove the ovary.
After surgery, in order to prevent relapses, a woman is recommended to carefully monitor her reproductive health, protect herself from stress overload, and try to prevent disruptions in the functioning of hormones.
Treatment of follicular ovarian cyst
Methods:
- Observation. Sometimes the neoplasm does not need to be treated, it goes away on its own, but the patient should be under constant supervision of doctors who will determine what the cyst looks like using ultrasound.
- Physiotherapy. This method of treatment helps to create conditions for the regression of cystic formation. Modern devices are capable of delivering medications to the required areas of the body painlessly and without injuring the digestive system (electrophoresis, ultraphonophoresis, magnetic therapy).
- Oxygen therapy. It is used when the patient experiences stress as a result of the periodic return of the disease. The method has a beneficial effect on brain activity, helping to reduce emotional stress.
- Hormonal and anti-inflammatory treatment. The method involves recommendations for taking oral contraceptives, anti-inflammatory drugs and vitamins.
- Homeopathic and traditional treatment. When the size of the cystic formation does not exceed 5 cm, it can resolve spontaneously. To support the body and to speed up the process, you can use homeopathic and folk remedies.
- Surgical intervention. Surgery will be required if PKJ cannot be cured with medications; it continues to grow. The intervention involves laparoscopy, removal or reduction of the size of the ovarian walls, and enucleation of the cyst.
How is cystic formation treated?
To get rid of cystic formations of the left ovary, a complex of medications is used, which includes the following groups of drugs:
- hormonal (prescribed individually based on tests);
- anti-inflammatory (Ibuprofen, Voltaren);
- antimicrobial;
- immunostimulants (vitamins A and E, folic and ascorbic acid);
- sedatives (Notta, Novo-Passit, Valerian);
- folk remedies.
Is it possible to get pregnant with a functional cyst?
Many women are concerned about the question: is it possible to get pregnant with a follicular ovarian cyst? Experts say that with this disease, infertility may occur while the tumor is resolving.
When only the left ovary is affected, the right one can release an egg that can be successfully fertilized conventionally or through IVF. Follicular cystosis and pregnancy are not uncommon today, but their proximity is an exception to the rule.
In most cases, cystic formation begins to regress during fertilization.
Why are functional ovarian cysts dangerous?
Functional cysts located inside the left ovary are dangerous due to possible complications:
- twisting the leg;
- hemorrhage into the peritoneum or ovary;
- wall rupture.
Source:
Functional cysts of the right and left ovaries
Functional ovarian cyst is a common disease in gynecology, the presence of which many women are not even aware of. The problem has not been considered a rarity for a long time; mechanisms have been developed for how to treat it and for a woman to undergo rehabilitation after therapy.
In most cases, a benign formation does not pose a danger to a woman’s health, but in the presence of certain factors it can turn into a serious threat. Women are actively studying what it is, the symptoms of the disease, the mechanism of its appearance and development, this knowledge helps them realize the potential danger.
Benign lesions can appear and disappear on their own. Sometimes a woman doesn’t even know about it. Large cysts that compress the ovaries and nearby organs pose a potential danger.
What it is
A benign formation that forms after the egg has matured is a functional cyst.
As a rule, it has smooth walls and a rounded surface. Its dimensions may vary in each individual case. More often its diameter is a couple of mm. In rare cases, during an examination, the doctor diagnoses the presence of a cyst up to 20 cm. Such neoplasms pose a threat to the health and life of a woman.
A cyst of the right and left ovary can resolve on its own, the woman will not even know about it. This is typical for formations of small sizes and occurs within 2-4 full menstrual cycles.
When a large cyst is diagnosed, the gynecologist decides on the treatment method. It is already dangerous for a woman’s reproductive health. As it grows, the surrounding tissues are compressed. As a result, pain and discomfort occurs.
Causes and risk factors
Women are interested in why a functional cyst occurs and what affects its development.
The main reason for the formation is considered to be a hormonal imbalance and an increase in estrogen levels.
In addition, related factors are:
- Disruption of the functioning of the endocrine system, pathological diseases of the thyroid gland.
- Previous infectious diseases of the reproductive system, STIs.
- Abortion.
- Trauma to the reproductive organs.
- Incorrect use of COCs.
- Frequent use of emergency contraception.
- Regular heavy physical activity.
- Stress.
- State of chronic fatigue.
It is worth remembering that the greatest stress for the female body can be a sudden change in climate, fasting, vegetarianism, or a strict diet. The functioning of the reproductive system is negatively affected by obesity. Estrogens are actively produced from adipose tissue, which causes their excess.
Surgery to remove one ovary causes too much estrogen to be produced.
Age-related changes in girls during the establishment of the menstrual cycle and in women during menopause can cause the formation of cysts. Under special supervision of doctors are nulliparous women and those who gave birth to a child after 35 years. This group includes those who have not had sexual intercourse.
Gynecological practice shows that cysts most often form on the left ovary.
The formation of a follicle with an egg that has matured more often occurs in it and, accordingly, the follicle ruptures more often.
Another reason is the proximity to the small intestine, which can be a source of infection. The formation often appears on the right ovary in women of reproductive age.
Types of functional formations
Functional cyst in gynecology has 2 types:
- Luteal. Its growth begins after the egg leaves the follicle, leading to the fusion of its walls, where fluid accumulates. Its second name is corpus luteum cyst.
- Follicular. Its development occurs when the follicle does not burst after the end of the egg maturation process. Fluid begins to accumulate inside and an egg remains. Gradually the follicle transforms into a cyst.
Source: https://cmsch71.ru/mammologiya/funktsionalnaya-kista-pravogo-i-levogo-yaichnika-chto-eto-takoe-i-kak-lechit.html
Functional ovarian cyst: symptoms
Functional ovarian cysts are usually asymptomatic. In this regard, they can only be detected during a bimanual vaginal examination, provided that the cyst reaches a certain size.
Despite the hidden symptoms, functional ovarian cysts may have the following clinical picture of the disease:
- Moderate pain in the lower abdomen. Luteal cysts, unlike follicular cysts, are more often accompanied by painful sensations;
- Minor spotting in the middle of the cycle;
- Amenorrhea is the absence of menstruation in a woman for six months;
- Disorders of the pelvic organs: dysuric phenomena and intestinal dysfunction;
- Infertility.
Possible ovarian diseases and their symptoms
Inflammatory diseases
First of all, these include oophoritis, which is one- or two-sided in nature. It often occurs simultaneously with salpingitis. When the fallopian tubes and ovaries are affected, we are talking about adnexitis.
Manifestations of oophoritis (in acute form):
- severe pain in the lower abdomen,
- fever,
- headache,
- frequent urge to painfully empty the bladder,
- unusual and heavy discharge,
- digestive disorders,
- bleeding between periods
- pain during intimacy,
- difficulty falling asleep, nervousness, increased fatigue.
Chronic pathologies
These ovarian diseases occur due to untimely or improper treatment. As a rule, they are protracted and occur with periodic exacerbations, during which the following occur:
- nagging and prolonged pain in the vagina, lower abdomen and appendages,
- cycle disorders,
- scanty whitish discharge from the genital tract.
Symptoms intensify before menstruation, against the background of hypothermia and colds.
Ovarian exhaustion
Such problems with the ovaries are often detected in women under 45 years of age. The following symptoms occur:
- irregularity of the menstrual cycle, and, ultimately, a complete absence of menstruation,
- hot flashes, sweating, which are more often observed after stress, during changes in ambient temperature, after a hearty lunch,
- psycho-emotional problems,
- dryness of the vaginal mucosa,
- thyrotoxicosis,
- dullness and brittleness of hair,
- the appearance of wrinkles on the face and hands,
- sometimes – hyperandrogenism, metabolic disorders.
Cyst formation
Often ovarian cysts do not manifest themselves. Sometimes a pain syndrome occurs, which is aching or pulling in nature, localized on one side, and intensifies during intimacy. In case of rupture or torsion of the cyst, it becomes pronounced, spreads throughout the abdomen, migrates to the rectum, and is accompanied by nausea and vomiting.
Women with ovarian formations sometimes experience cycle disturbances (delayed menstruation or dysfunctional uterine bleeding). An enlarged abdomen is observed only with tumors of impressive size.
Multifollicular ovaries
In pathology, paired organs contain multiple immature follicles. This condition of the appendages is sometimes normal, but often precedes polycystic ovary syndrome. If multifollicularity is pathological, then the menstrual cycle is disrupted.
Polycystic ovary syndrome (PCOS)
This disease is accompanied by the following symptoms:
- long delay or absence of menstruation,
- male pattern hair,
- oily skin and hair,
- irritability, tearfulness, depressed mood,
- pain in the lower abdomen,
- acne,
- infertility.
Ovarian cancer
Oncological tumors often form in patients over 40 years of age. Women who have not given birth, as well as people who have had abortions in the past, are at risk. In the early stages, the pathology is sometimes mistaken for adnexitis, because cycle disruptions and pain in the lower abdomen are observed. As it progresses, the state of health worsens and the functioning of the stomach and intestines is disrupted.
Apoplexy (rupture) of the ovary
During the abnormal process, the walls of the organ burst, resulting in hemorrhage into the peritoneum. In this case, the woman feels weakness, dizziness, fever, and severe pain. The trigger for apoplexy can be: active intimacy, abdominal injury, inflammatory process in the pelvic area.
Ovarian hyperplasia
The disease occurs as a result of the proliferation of the endometrium and stroma. This leads to swelling of the appendage. Hyperplasia is congenital or develops against the background of hormonal imbalance. Its dangerous complication is tecosatosis.
Signs of hyperplasia:
- earlier or later onset of the menstrual cycle,
- infertility,
- bleeding between periods
- irregular cycle,
- cystic follicles,
- hormonal imbalances that provoke weight gain, excess body hair growth, etc.
Psychosomatic diseases of the appendages
Psychosomatics considers the ovaries as centers of creation and creativity. If you do not accept your femininity and do not want to treat yourself as a continuator of the family, disturbances in the functioning of paired organs occur. A woman thinking about what to do if her appendages hurt should think about psychosomatic factors.
Thus, adrenogenital syndrome, in which the adrenal glands are activated and the production of male sex hormones is launched, develops as a result of an attempt to take on male functions. The body rebuilds itself and begins to produce many immature follicles. In this case, PCOS develops.
Functional ovarian cyst: diagnosis
Approximately 70-80% of all functional ovarian cysts resolve on their own and do not require conservative or surgical treatment. In other cases, if a cystic formation is suspected, the woman should make an appointment with a specialist. Diagnosis of functional ovarian cysts is made on the basis of a gynecological examination, ultrasound diagnostic data of the pelvic organs and laparoscopy. When conducting a bimanual vaginal examination, a tumor of a round shape, tight-elastic consistency and a smooth surface is palpated on the side and in front of the uterus. The cyst is mobile and not fused to the surrounding tissues.
Ultrasound scanning visualizes a spherical single-chamber formation of 3-9 cm in diameter, filled with homogeneous anechoic (non-reflective ultrasound) contents. In unclear situations, diagnostic laparoscopy is resorted to.
Functional ovarian cyst: treatment
If the ovarian cyst is small in size (up to 5–6 cm in diameter) and is asymptomatic, then in these cases the patient is monitored dynamically with ultrasound monitoring of the state of the reproductive system every month.
Treatment of functional ovarian cysts involves the combined use of both conservative therapy and surgical removal. To stimulate the reverse development of ovarian cysts, combined oral contraceptives, anti-inflammatory drugs, vitamins, and homeopathic remedies are used.
At the Yusupov Hospital there are a number of innovative methods for treating functional ovarian cysts. Treatment with duphaston allows you to effectively cope with cystic neoplasms of various etiologies, which pose a danger not only to a woman’s reproductive function, but also to the development of malignant tumors.
Surgical removal of an ovarian cyst is performed in cases of persistent form and progressive increase in formation (cyst diameter greater than 8 cm). In typical cases, laparoscopic enucleation of the cyst with suturing of the walls or resection of the ovary is performed.
Yusupov Hospital is a multidisciplinary center created according to international standards of service quality. Each clinic specialist works within the framework of evidence-based medicine. Thanks to cooperation with foreign clinics, the hospital uses only European protocols for the treatment of various gynecological diseases. To make an appointment with leading Russian specialists, you just need to call.