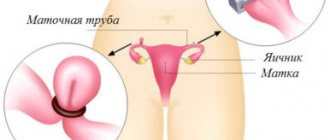
The uterine or fallopian tubes are also called oviducts, because it is their main function that carries the egg from the ovary to the uterus. The medial part of the tubes connects to the uterine cavity, and the lateral or ampullary part is located next to the ovaries. The ovaries together with the tubes are called the uterine appendages. After ovulation, the egg enters the abdominal cavity, where the movement of the villi of the ampullary part contributes to its forward movement into the lumen of the tube.
Unlike sperm, which can move against the flow of fluid, the egg is immobile. It is forced to move into the uterine cavity by the movements of the cilia of the mucous membrane and successive contractions of the muscle layer. Inflammatory processes, injuries and neoplasms lead to the formation of adhesions and scars that block the lumen and prevent the egg from reaching the uterine cavity.
Fallopian tube obstruction is a collective concept that includes the following pathological conditions:
- complete obstruction;
- obstruction of one pipe;
- partial obstruction due to impaired peristaltic movements;
- disruption of the ciliated epithelium.
Normal structure and functioning of the fallopian tubes
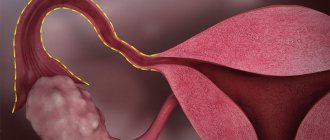
The fallopian tubes are thin tubes about 8-10 cm long. The wall of the fallopian tube consists of 3 layers - mucous, muscular, serous. The beginning of the fallopian tube originates from the wall of the uterus in the area of the angle and opens with the fimbrial section towards the ovary. The lumen of the fallopian tube expands evenly from the uterus to the ovary, representing a funnel. It is the fimbrial region that plays an important role in capturing the egg and guiding it through the fallopian tube into the uterine cavity. Only with the preservation of the fimbrial part of the fallopian tube, as well as the cilia of the fallopian tube mucosa, is it possible to transport the egg into the uterine cavity.
The egg is not endowed with the ability to move independently through the fallopian tube; only contraction of the fallopian tube and the synchronous movement of the cilia propel the egg into the uterine cavity. If the fimbriae are damaged by an inflammatory and/or adhesive process, then the epithelium may completely or partially lack the ability to capture the egg and move it along the tube. Damage to the ciliated epithelium greatly interferes with fertilization, significantly reducing its chances. Sometimes the fallopian tube is mechanically passable, and when performing tuboscopy, complete destruction of the ciliated epithelium of the fallopian tube is revealed. In such cases, we can talk about the occurrence of an ectopic pregnancy with an externally preserved and patent fallopian tube. In the case when the patency of the fallopian tubes is difficult or the cilia are not able to fully function, there is a possibility of an ectopic (ectopic) pregnancy.
Causes of fallopian tube obstruction
The reasons that lead to obstruction of the fallopian tubes include:
- endometriosis of the ovaries, fallopian tubes, ligaments of the uterus;
- adhesions in the pelvis;
- tubal infection;
- tubal ligation (sterilization).
Complete obstruction occurs when all or part of the pipe is obstructed. The reason for this diagnosis is often pelvic inflammation, which occurs due to a specific or nonspecific infection or external genital endometriosis. With endometriosis, the tissue lining the inner surface of the uterus grows in size outside its cavity. Endometriosis causes obstruction of the tubes and the formation of adhesions in them. With a high degree of development of endometriosis, the likelihood of the spread of adhesions also increases. Symptoms of endometriosis may not be severe in all women. If there is no heavy menstrual flow or the menstrual cycle is accompanied by cramps, the disease is difficult to diagnose. The presence of endometriosis can be reliably determined by laparoscopy.
Fallopian tube infections
Infection of the pelvic organs can occur due to the development of appendicitis or colitis, the presence of an infection in the intestines, or the presence of genitourinary transmitted diseases. Frequent douching can cause an infection in the pelvis, most of which is a nonspecific infection. A woman may not know that she has suffered a serious infection that has led to obstruction of the fallopian tubes. Only when trying to get pregnant does she learn about her illness during the examination process. The most common causes of infections in the pelvis are sexually transmitted diseases.
In past years, gonorrhea was most often detected, currently chlamydia. Repeated infections with chlamydia often lead to infertility due to obstruction of the fallopian tubes. But even a single case may be enough for the patency of the fallopian tubes to be lost.
Modern medicines can relatively easily cure gonorrhea and chlamydia, but the adhesive process in the pelvis cannot be corrected by medication. That is why, when diagnosing infertility, the doctor prescribes a test to detect these infections not only by PCR, but also by determining antibodies in the blood.
Women who do not have infections in the pelvic organs may still experience adhesions in the ovaries and fallopian tubes. Their appearance can be caused by surgery on the ovaries or other abdominal organs, that is, an adhesive process of postoperative origin develops. The likelihood of adhesions increases if the operation was extensive or complicated by infection, accompanied by the placement of drains in the abdominal cavity. For example, a ruptured appendix, massive intra-abdominal bleeding. The sperm may not meet the egg on its way even if the tube is slightly deformed. The likelihood of an ectopic pregnancy also increases.
Expert opinion of a doctor
Litvinov Vladimir Valentinovich
Reproductologist, obstetrician-gynecologist, Ph.D. Normally, fertilization occurs in the ampulla of the oviduct, within 24 hours after ovulation. Moving through the lumen of the tube, the fertilized egg continues to divide and, once in the uterine cavity, it becomes a blastocyst, which, under favorable conditions, penetrates into the endometrium of the uterus, and this is how implantation occurs. Otherwise, if fertilization does not occur, the egg dies.
Diagnosis of fallopian tube patency
To investigate possible causes of infertility, it is very important to conduct a tubal patency test, since tubal factor infertility is common. Tubal patency is determined by two methods: hysterosalpinography and diagnostic laparoscopy.
Hysterosalpingography or metrosalpingography (HSG or MSG) refers to x-ray examinations. A special contrast agent is injected into the uterus, which helps visualize the internal state of the uterine cavity and fallopian tubes. To exclude the possibility of irradiation of the fertilized egg, this X-ray examination is performed immediately after the end of menstruation. When performing hysterosalpingography in this menstrual cycle, it is not advisable to plan a pregnancy.
Hysterosalpingography is performed without anesthesia under local anesthesia. You only need to take a small dose of anesthetic intramuscularly or perform a paracervical blockade. This will relieve discomfort, and the x-ray procedure will cause at most minor cramping. To reduce the risk of infection in the abdominal cavity, some doctors prescribe antibiotics. The results of HSG will make it clear how passable the tubes are and whether the condition of the uterine cavity is normal. However, the accuracy of this method is only 83%.
Medical practice shows that HSG can lead to pregnancy in the first few ovulation cycles. This is explained by the washing effect of the injected contrast solution. Hysterosalpingography today is one of the most important stages of the initial examination for infertility. The patency of the fallopian tubes is also checked under ultrasound control. This procedure is called sonohysterosalpingoscopy (SHSS). It is similar to HSG, but excludes irradiation of the pelvic organs, since instead of a contrast agent, a sterile saline solution is injected.
The disadvantage of ultrasound of tubal patency is its low reliability, since the X-ray machine is much more accurate than the ultrasound machine. Although X-rays can accurately assess the patency of the tubes and the condition of the uterus, they do not provide a sufficient understanding of the adhesions and foci of endometriosis, which can cause infertility.
The outer surface of the fallopian tubes is better assessed by laparoscopy. This study complements the results of GHA and is performed under general anesthesia. An endoscope, a small optical medical instrument, is inserted into the abdomen through an opening in or near the belly button. The doctor uses a laparoscope to examine the ovaries, uterus, tubes, and examine the peritoneum and abdominal cavity. The colored substance that flows through the cervical canal into the uterus and fallopian tubes indicates whether they are patent. To perform surgical manipulations, additional surgical instruments are introduced into the pelvic area through an incision in the pubic region through 3 mm punctures. During laparoscopy, it is possible to dissect adhesions, remove ovarian cysts and uterine fibroids, and shaving (excision) of foci of endometriosis.
Causes
Tubal obstruction includes the following conditions:
- obstruction of one tube
- complete obstruction of 2 pipes
- partial obstruction (which can cause improper implantation of the fertilized egg)
- adhesions around the appendages
- dysfunction of the villi, which move the egg released from the ovary into the fallopian tubes
If the adhesions press on the outside, or if there is a blockage inside the tube, this still means infertility. The causes of obstruction of the oviducts may be as follows.
Inflammation of the appendages
The inflammatory process in the uterine appendages can be acute, subacute, hidden (latent). Mild symptoms may occur with:
- cytomegalovirus
- mycoplasmosis
- chlamydia
- ureaplasmosis, etc.
When the inflammatory process is acute, the woman is treated in the hospital, using anti-inflammatory drugs that destroy the causative microbes. Then follows a course of recovery and treatment for resorption. When pathological bacteria multiply, the products of their activity accumulate inside the fallopian tubes. There is also an accumulation of purulent masses and mucus. If this condition is not treated in time, scar tissue grows on the walls. Adhesions form, resulting in obstruction of the fallopian tubes.
Tuberculosis of the genital organs
This is a very rare rather than common cause of infertility. Tuberculosis pathological process in the genital organs of women is rarely diagnosed. But today the population in general has decreased resistance to mycobacteria, which is why this cause of infertility should be considered when diagnosing a patient. In recent years, the incidence among children has increased. Almost all people become infected with Koch's bacillus before the age of 20. But the disease does not make itself felt immediately; years or even decades may pass before any clinical manifestations appear.
Tuberculosis affects not only the lungs (not everyone knows about this). Any organs can be affected, but there will be no obvious symptoms. And diagnosis is very difficult, because it is difficult for doctors to suspect that the cause of the disease is mycobacterium tuberculosis.
When a girl whose genital organs are just developing is infected, the uterus and appendages grow incorrectly, the balance of hormones in the body is disrupted, hypomastia is formed, and the fallopian tubes are blocked. Ovarian function may be impaired in such cases.
After infection, the immune system overcomes the tuberculosis pathogen, and foci of inflammation self-destruct without treatment. When immunity decreases due to some circumstances (the body is exhausted, a person is on a diet, experiences stress, enters puberty, etc.), the disease can worsen again. After all, it will be difficult for the body’s defenses to cope with the raging mycobacterium. X-ray will not show anything, because the process affected not the lungs, but the genitals.
In the CIS countries today, the problem of increasing tuberculosis incidence statistics is not taken into account. They also do not take into account that many forms of the disease are resistant to previously used drugs. Diagnosis of extrapulmonary forms of tuberculosis is at a catastrophically low level. This is often an obstacle to conception.
TB services do not receive enough funds. If a person turns to them, then the most familiar methods are used for diagnosis, which are mainly aimed at detecting a pathological process in the lungs. There is also a shortage of highly qualified doctors—phthisiologists-gynecologists—in many cities. Culture for mycobacteria for genital tuberculosis in females can give a negative result (and it will be false).
You should contact the gynecological department for examination for extrapulmonary tuberculosis if:
- constantly or in the 2nd phase of the cycle, a woman’s temperature remains at 37-37.5 degrees
- I have allergies
- feeling weak
- there is salpingoophoritis or salpingitis that occurs chronically
- increased sweating
- negative results when tested for hidden infections
- violations of the cycle of critical days
- obstruction of the tubes leading to infertility
- uterine hypoplasia
- no effect of treatment
Other reasons
There are also such reasons that provoke obstruction of the fallopian tubes:
- endometriosis
- surgical intervention in the pelvic organs or abdominal cavity (for adhesions, peritonitis, trauma to the abdominal area, intestinal pathologies that are treated surgically, etc.)
- polyps or tumors in the fallopian tubes
- abnormalities of tubal development inherent in the patient from birth
- history of ectopic pregnancy (ectopic)
- abortions with complications, tubal hydrotubation, intrauterine procedures, etc.
If the inflammation in the appendages is acute, with obvious symptoms, the doctor may prescribe surgical removal of a tube or two at once. Therefore, pregnancy will no longer be possible, unless artificial insemination methods are used. Also, those who are unsuccessfully treated for infertility should not forget about the possibility of adopting a child. By doing this you will not only achieve your goal, but also do a good deed.
Hysterosalpingography images
The right fallopian tube is obstructed in the ampullary section.
The left fallopian tube is freely patent.
The "R" on the image indicates the patient's right side.
The arrow indicates an obstruction in the ampullary section of the right fallopian tube.
The right and left fallopian tubes are difficult to pass due to the presence of bilateral valve sactosalpinxes.
The image clearly shows dilated and tortuous fallopian tubes.
The arrow shows the fallopian tube on the left with the presence of a valve sactosalpinx.
The "R" on the image indicates the patient's right side.
The left fallopian tube is freely patent.
The right fallopian tube is obstructed in the intramural section.
The arrow indicates the presence of an obstruction at the mouth of the right fallopian tube.
The letter "R" in the image represents the patient's right side.
The left fallopian tube is obstructed in the ampullary section.
The right fallopian tube is difficult to pass due to the presence of a valve sactosalpinx on the right.
The arrow shows the valve sactosalpinx on the right.
The "R" on the image indicates the patient's right side.