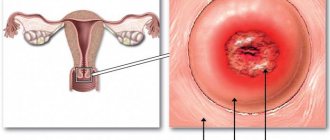
Cervix in everyday life
The average menstrual cycle for a woman is 28 days. The normal state of the cervix is tight and closed. Color: light pink. During the period of ovulation, which occurs on days 13-15 of the cycle, it softens and the cervical canal expands. The level of the female hormone estradiol increases significantly before follicle rupture, the body prepares for fertilization. All these changes occur for better passage of sperm to the uterus, where the egg may already be located.
You need to remember that a soft cervix in a healthy woman in the middle of the menstrual cycle is normal!
After ovulation, the cervix remains soft for several days, regardless of whether fertilization has occurred or not. After which the cervical canal narrows, and the organ itself becomes dense.
Reasons for deviations from the norm
There are a number of reasons why the structure of the cervix may be disrupted.
It can be:
- The first weeks of pregnancy.
- The period after and before childbirth.
- Difficult previous labor with multiple ruptures.
- Congenital abnormalities.
- Reduced muscle tone of the cervix (isthmic-cervical insufficiency). The occurrence is promoted by both mechanical damage and hormonal disorders.
- Inflammation of female organs. Often this is the cause of female infertility.
- Previous abortions.
- Hormonal imbalances.
- Taking medications.
Asymptomatic reduction in length and dilatation of the cervix
Isthmic-cervical insufficiency (ICI) is a premature asymptomatic decrease in the length and dilatation of the cervix, which can lead to premature birth. This can happen in the second or early third trimester of pregnancy. As the baby grows, its weight puts more pressure on the cervix, and if it is soft, weak or too short, then there is a possibility of giving birth soon. In this case, there may not be any spasms or other symptoms of upcoming labor.
Are short cervix and isthmic-cervical insufficiency the same thing?
No, a short cervix and ICI are completely different concepts. A short cervix refers only to the length of the cervical canal. On the other hand, ICI refers to the premature thinning of the cervix and the widening of its canal when the muscles of the uterus and its cervix are unable to remain rigid and strong. However, cervical insufficiency can lead to a short cervix.
The first weeks after fertilization
After the fertilized egg attaches to the uterine cavity, the complex process of restructuring the circulatory system necessary to nourish the fetus begins. The ovaries, under the influence of the corpus luteum, begin to produce more and more progesterone, which is responsible for the texture of the cervix. The cervical canal closes and is filled with mucous contents. This provides protection to the membranes from various bacteria. The cervical spine itself becomes dense after a few weeks. This keeps the growing fetus in the uterus.
But it happens that a soft cervix during pregnancy in the first trimester is a reason to take medications. Your doctor may prescribe hormone therapy. Preparations containing progesterone are usually prescribed.
Pregnancy and “No-shpa”
A doctor may also prescribe “No-spa”. During early pregnancy, there may be a risk of miscarriage due to the tone of the uterus. Drotaverine, which is the active ingredient in No-shpa, relaxes smooth muscles and relieves spasms. It does not pose any danger to the fetus. The drug is completely eliminated from the body within 24 hours.
In the case of headaches and toothaches during early pregnancy, “No-spa” can act as a painkiller. For problems with the gastrointestinal tract, you can also use this drug, but only after consulting a doctor.
Softening of the cervix in the second trimester
During pregnancy, periodic stretching in the lower abdomen is not a deviation from the norm, unless it is periodic. In this case, a doctor's examination may be necessary, since this is the only way to determine a soft cervix. It is possible to diagnose her condition yourself, but it is a very risky procedure.
A soft cervix during pregnancy at 20-30 weeks threatens premature birth or miscarriage, therefore, depending on the degree of softening and reasons, the doctor prescribes:
- bed rest;
- hospitalization;
- installation of a pessary;
- suturing;
- appropriate drug treatment.
Pessary placement and suturing
The most frightening thing for a woman on this list is the pessary and stitches. And this is natural, since any intervention carries a percentage of risk. But this is precisely what allows you to maintain the pregnancy and carry the child to term.
The procedure for installing a pessary, or Meyer ring, is painless and takes about 30 minutes. This is not a surgical procedure, so there should be no feeling of fear.
An obstetric pessary resembles a soft rubber ring made of surgical silicone or plastic. Its purpose is to relieve the uterus, which is under a lot of pressure. The doctor inserts it into the vagina and places it on the soft cervix. In everyday life, this device does not interfere with the woman in any way and is not felt inside.
The Meyer ring is worn almost until childbirth. The pessary is removed in the maternity hospital at 38-39 weeks.
Stitching is performed only under anesthesia, so the woman does not experience any pain. The optimal period is 23-25 weeks. Before suturing, a thorough examination of the internal genital organs is carried out. Only experienced doctors are allowed to perform this procedure, so the expectant mother does not need to worry. The risk of complications in this case is minimal, but the chances of a happy completion of the pregnancy are quite high.
Stress has a big impact on the cervix. That is why a pregnant woman needs to be protected from negativity and surrounded with care. The expectant mother needs to spend more time in the fresh air and devote sufficient time to physical activity. Reading, as well as watching positive films and programs will help improve your mood.
There has long been controversy regarding maintaining bed rest. It has already been proven that walking does not affect the smoothing and softness of the cervix. And constant lying down is fraught with other unpleasant consequences in the form of excess weight and weakened muscle tone. If you trust your doctor, it is better to discuss this issue with him and listen to his opinion and your own feelings.
smoothed cervix during pregnancy
The PDR passed, and the days dragged on like rubber - every minute was filled with anticipation: when will it be, when?
Any pain or just discomfort in the abdomen - and I began to listen to myself: has it started? No, it hasn't started...
At night, these sensations mixed with dreams where I was supposedly having contractions, and when I woke up, I tried for a minute to understand where the dream was and where reality was. But morning came and I was still “deeply pregnant.” All my friends whose due date was approaching wanted to give birth, for many the desire turned into attempts at self-stimulation - washing floors, running up the stairs, drinking various wines - dry and sparkling, even dates were used, and some, the most desperate, wondered: “What is the probability that after castor oil gives me a headache, I will give birth?” The probability was quite high, but also just as unpleasant, so I tried not to succumb to mass hysteria and distract my head with household chores, taking my husband on forced walks so as not to lie too long.
So that day, January 23, I went to the hospital on foot. The midwife examined me, determined that my cervix was smooth and half a centimeter dilated, and told me to wait for the birth to continue. Well, what could I do? In the evening, my sister and I made another circle around the city at a brisk pace (although how can we still do in such cold weather), everyone was looking for popcorn for the microwave for the evening movie show, but we couldn’t find it. We took some seeds. Eh, I had to gobble up chocolate, it was the last few hours left!
At home, my husband and sister started watching a film with the sacred title “Tinker Tailor Soldier Spy!”, perhaps this influenced the onset of labor.
At 22:30 I felt pain in the lower abdomen, similar to menstrual pain. I’ll add that I didn’t have any precursors (the removal of the plug, training or false contractions) before this. So I decided to check the contractions - maybe they were training contractions. I started counting the intervals, but got distracted by the movie and got confused. As a result, during the next contraction I fidgeted, and my husband saw through me: “What happened?” “I don’t know yet, maybe the contractions are real, or maybe they’re false.” We began to count the intervals together, but they were different each time - sometimes 10 minutes, then 14, then 8... As a result, while we were counting, such a noticeable contraction came that my husband said: “Get dressed, let’s go!”
We are about 100 km from the maternity hospital, all the bags had been packed for a month already, I just braided my braid tighter, and we left. It was 00:40 on the clock. We drove for about an hour and a half and counted the intervals the whole way. Now the contractions were established with an interval of 6-7 minutes, but they were quite tolerable, I practiced my breathing a little. We arrived at 2 am, the nurse in the emergency department glanced sideways at my big belly and asked: “What are you complaining about?” and after listening to the story about my contractions and intervals, she sent my relatives home with my clothes, and I, having changed into a nightie, robe and slippers, began asking questions and filling out documents. Then she examined me (I shaved myself) and sent me for an enema (a quite tolerable procedure).
Then we went to the doctor with another nurse and my things, she looked at me in the chair, the dilation was 1 cm. She said that it was still a long time before the active stage, and suggested medicated sleep. I refused. The nurse took me with my things to the delivery room and when I asked when I would give birth, she answered: “Well, around lunchtime!” Next, she laid me on the couch and installed a device for measuring CTG. The CTG recording lasted about an hour, all this time I was breathing through contractions, noting them on the device’s clock - an interval of 6 minutes. Afterwards we went to the doctor again, she punctured my bladder (a completely painless procedure), and I returned to the couch to breathe. The nurse once again suggested medicated sleep (“rest, otherwise you won’t have the strength to give birth”), but I again refused and confirmed this in writing.
I would like to add that throughout the labor, both “inactive”, that is, from arrival until 6 o’clock, and “active”, that is, from the beginning of strong contractions, I was alone in this large hall, the staff was in the neighboring rooms. This was surprising to me, for some reason I thought that throughout the birth I would be surrounded by people in white coats and even holding my hand, but so I lay alone on the couch and groaned, “breathing out” the contractions with all my might, the nurse only occasionally came to see how I was giving birth there. When the doctor came and looked at the dilation, it was 4 cm. For me, this is not much, but the nurse said that it was very good - 3 cm in 2 hours and I am one of those who give birth well. At this point I was happy, but it was too early.
In general, I gave birth like this until 6 in the morning, the contractions were strong but tolerable, I also corresponded with my husband via SMS, managed to take a nap between contractions, and at 6:00 the nurse said that the “active phase of labor” was beginning, now I had to get up and walk for 2 hours. She suggested that I take a shower, but I decided that as long as the contractions were tolerable, I would not use this bonus, and scheduled a shower for myself at 7. In general, I felt comfortable knowing what was happening and how long it would last - it gave the impression that I was in control of the situation, so It was easier for me to distribute forces and navigate in time. The fact is that an hour later there was a shift change, and unlike the previous shift, the medical staff of which told me everything in detail, no one really explained anything, and I didn’t understand what was happening, how long it would last, I was seized with panic and I think because Because of this, I got into trouble that could have been avoided. I walked all flushed around the ward in circles, during contractions I tried different positions - I didn’t like kneeling, I didn’t even try the ball, leaning on the windowsill would have been nice, but there was a fire-breathing radiator under it, so I went out into the corridor (where at least it was a little cooler) and leaned on the table, or even more I liked the pose with my hands against the wall, while I rocked my pelvis from side to side, as the nurse told me, in order to prepare it for childbirth.
The contractions intensified, everything swam before my eyes, I looked at the clock and waited for 7:00, for which I had scheduled a shower for myself. At 7, I had already undressed with difficulty and crawled into the cabin, not to say that the water brought real relief, but it was some kind of variety, although a friend said that she felt much better in her soul. The nurse said that during a contraction, direct a stream of water to the place where the pain is concentrated - in my case, the lower abdomen. I poured water on myself from the shower, the intervals between contractions became shorter and shorter, but I didn’t like directing the stream to my stomach - it hurt so bad there, and I also poured a warm shower on it, as if to accentuate the pain... In general, I waited out the contractions, hunched over like a comma and looking like a stream watering my feet.
The main thing I realized during childbirth is that the ways to “survive” a contraction are very individual. First of all, in order to wait out the fight, two components are needed - posture and thoughts. That is, you need to choose a position in which you can realistically wait for the end of this pain, and the appropriate thoughts to occupy your head with something - something like a mood: words that will help you abstract yourself until the end of the fight. Moreover, both posture and thoughts will need to be changed over time, adapting to the growing contractions. That is, if at the beginning I waited out the contractions lying down, distracting my head by reading prayers from a book, then later I could not read, and the postures became standing and “leaning.” Concentration on breathing is also good for distracting your head; I didn’t use any specific technique I read on the Internet, I just breathed deeply. When the contractions became the strongest, I curled up (and somehow on one side, it was easier for me), and “distracted” my head, imagining that I was just swimming in an ocean of pain and looking for the shore... searching... searching... phew, the end contractions.
When I dried myself off and left, a new midwife and a nurse were already there, they looked at my dilation - 6 cm, and told me to walk. I walked for about half an hour, and either the shower had worn me out, or the sleepless night had taken its toll, but I really wanted to sleep. I lay down on the couch and, despite the strong contractions, I even dozed off a little when the nurse came and cursed why I was lying down, she told me to walk, to which I replied that I was just lying down. She didn’t really believe it, she told me to get up and walk (don’t lie still) and left, but I really didn’t want to get up, it seemed like there was nothing better than just lying down and dozing... but with an incredible effort of will, I still forced myself to get up and walk around. It was so hard, I had no strength at all, and the couch was right there!
Having made two circles around the ward, I lay down on the couch again. And then of course the nurse came in. “Are you still lying down? I told you to go!” “Well, I just lay down, really...” “Yeah, of course”... I didn’t have the strength to laugh, so I just whined that it was so good to lie down and I wouldn’t get up. She left and came with a doctor, who told me to give me stimulation. Apparently, they were afraid that I would completely lose my strength or the contractions would fade away, or maybe they just wanted to quickly get rid of the “remnants” of the previous shift, in general, they put me on an IV, told me to lie down and not bend my arm, plus they injected some other medicine into it , I think a painkiller, and they left, saying: “As soon as the contraction begins, breathe deeply, through elongated lips, and as if you are inflating a balloon as you exhale.”
Literally a minute later, the contractions became more frequent and intensified, I was rushing around the couch, forgetting about breathing, at the peak of the contractions I could no longer stand it and, to my shame, I began to scream, although before the birth I had prepared myself and promised myself, firstly, to breathe correctly and, Secondly, don't shout. A nurse came and I asked to take out the IV, she looked at the “bag” - it seemed that only a tenth of the entire liquid had dripped out from there, and said: “Lie down, not much has dripped yet,” she tried to joke, but I stared into nowhere with sightless eyes and didn't react to her. Well, how long will this continue!
The doctor came and said the dilation was 8 cm, we are still waiting, I thought that at 8 it was already possible to give birth, why didn’t they put me on the table, I again screamed from the contractions, practically losing control over myself. Still, it was a thrill to shout. When you endure, endure, and that’s all - you scream because you can’t anymore, then you let go a little, so I think there’s nothing wrong with a little screaming.
As a result, a nurse came and, seeing that I was feeling very bad, said: “Why are you still lying there? Come on, I’ll show you how it will be easier for you.” She picked me up and took me to the toilet, where I really felt better. “Here,” she said, “sit on the toilet, but as soon as the contraction comes, get up!” I sat down on the toilet. What a relief it was, sitting on the toilet became much better, during the contraction I stood up, if you can call my crooked figure “standing up” with my leg bent almost to the floor. Apparently, after sitting on the toilet, I was so encouraged that I pulled myself together again and promised myself not to scream and to breathe correctly, and I succeeded.
So several contractions passed, when suddenly something uncontrollable swept through my body - as if I had gone to the toilet against my will or something... I don’t know how else to describe it, but I realized that it was an effort, and I screamed to the nurse about it. She came and took me back to the delivery room. As a result, I found myself back on the couch, the nurse told me, lying on my back, to grab my legs and, waiting for a contraction, to push “in the butt.” All this, together with pushing, was supposed to help my baby be born.
I should have practiced at home, but now I couldn’t do it, the efforts were mostly in the face, I was inflated like a balloon (although I had heard a lot of stories about pushing “in the face” - about burst blood vessels on the face and red eyes), but nothing I couldn't help it. Half of the efforts were in vain, the strength was becoming less and less. The time was around 10 am. It seemed to me that I would never give birth. If I knew that in 15 minutes the baby would be with me, I would have gathered my strength, but for the second time I lost control and let everything take its course.
However, apparently the shouting of the staff had an effect, because I felt something pressing on my crotch - it was already “knocking” on the top of my daughter’s head. And while I was chasing her back and forth, the doctor said: “The dilation is complete, run over to the birthing chair.” Everything was already laid there, the nurse raised it to the required height, raised the handrails, which I grabbed, rested my legs on special supports and told me to push as the contraction came.
I tried, but it came out every time. In the end, I decided to try harder, I remembered the advice about breathing while pushing: “If the contraction is still going on, and the breathing has run out, don’t give up, take in more air and push.” That’s what I did - I grabbed more air and continued to push, forgetting about the main thing: if the contraction was still going on... It cost me a first-degree perineal rupture. By the way, by the time I was on the birthing chair, there were about 4 staff. “Get used to the pain... breathe...” the midwife said, I began to breathe quickly. Strangely, the pain from the breakup quickly disappeared. The nurses ran in: “What are you doing, well, push!” Your child is suffering!” Still pushing, I pushed and screamed from the effort. A chest cry, some kind of bestial cry, this is the kind of moment that is probably shown in films when someone gives birth - you are not screaming from pain, from superhuman effort. Together they began to press on my stomach - once, and my daughter’s whole body came out of me, how pleasant it was, as if something warm had slipped out, and the pain immediately went away. Oh, how nice it is, is it really all over!..
The nurse picked up the blue, wrinkled baby, took it to wash and immediately placed it on my chest. The stories I read about this (“when my baby was placed on my chest, I forgot about the pain, it was the most beautiful moment in my life...”) did not come true for me, and without much emotion I pressed the “hedgehog” to my chest, I myself lay in some kind of prostration, exhausted both physically and mentally, with resentment towards everyone that they had not warned me and subjected me to such a test, in general, the state was not very joyful, and then my body began to pound in some kind of terrible shivering, I was lying literally bouncing on the delivery table, clutching my baby, wrapped in a diaper, to my chest. Meanwhile, the nurse took out the placenta, then they stitched me up. In general, that’s where it all ended, I lay on the chair for another 2 hours - I came to my senses, my baby was snoring under my side, and I asked the midwife to give me the phone and sent my husband photos of our daughter...
This is how my birth ended, for another day, as soon as I closed my eyes, pictures of past births flashed in front of me, I wondered how people can have more than one child in a family, who would voluntarily do this again?! I sadly said goodbye to the dream of a big family, but then the emotions subsided, after a couple of days I was able to remember it more calmly, after a week I thought “there was nothing special there...”, and after some time I wanted to repeat it . Yes, yes, I myself am surprised, but apparently Mother Nature made sure that all these negative memories were quickly erased from my memory. Now a little over a month has passed, and I’m already dreaming of a second child!
Childbirth is one day that we must give up from our lives so that our little ones can be there to grow and delight us every day throughout our lives. And let me tell you, it’s worth it!
Expert's comments
Upon admission to the maternity hospital, Lada was examined on a chair, reported that the cervix was dilated only 1 cm, and offered the expectant mother medicated sleep, explaining that she needed to gain strength for the active phase of labor. Despite the presence of more or less regular contractions, Lada had not yet experienced obstetric dilation (cervical dilatation during childbirth begins at 2 cm). Considering the full-term stage of pregnancy and the regularity of contractions, the doctor suggested that by the morning the expectant mother might go into labor (that is, contractions would intensify and the cervix would begin to dilate), so our heroine was hospitalized in the prenatal ward for observation. Medication-induced sleep, which was suggested to Lada, is caused by the administration of antispasmodic and sedative drugs to the pregnant woman; medications are administered intramuscularly or intravenously. It is used only during training contractions or at the very beginning of labor - during active contractions it is no longer effective. The main purpose of using medicated sleep is to enable the woman in labor to rest and gain strength before the onset of labor if precursor contractions bother her at night, do not go away on their own and deprive the woman of sleep. We can say that medicated sleep in this situation is the optimal means of preventing weakness of labor, the development of which in many cases is caused by a simple lack of energy in the woman in labor. Our heroine refused medicated sleep - probably guided by the desire to give birth naturally, without additional interventions. Lada also refused a few hours later, when the doctors suggested medication rest again. Unfortunately, in the case of our heroine, refusing the opportunity to rest at the beginning of labor was a mistake and later did Lada a disservice - her body did not have enough strength for active contractions, and labor had to be stimulated.
The contractions did not stop, but did not become stronger; The dilatation of the cervix also did not increase, so the doctor decided on the need for an amniotomy - puncture of the amniotic sac. The amniotic sac takes an “active part” in the process of childbirth: during contractions, it presses on the cervix from the inside, causing it to stretch and open. The fetal head, pressed against the cervix, divides the fetal waters into two parts: the “front” waters, located between the baby’s head and the wall of the bladder, press on the cervix, and the rest of the waters remain behind the fetus and protect it from excessive pressure of the uterus during contractions . Then, as the contractions intensify, the fetal bladder ruptures, the anterior waters pour out, the fetus presses its head against the cervix, stretches it completely and begins to move through the birth canal under the influence of contractions (the bladder ruptures on average at 5-6 cm of the opening of the cervix). If this does not happen, contractions weaken and the cervix stops opening; as a result, labor is delayed and the fetus begins to experience a lack of oxygen (hypoxia). To prevent the development of these complications, in the absence of dynamics of labor (increased contractions and increased dilatation of the cervix), the doctor performs an amniotomy. The amniotic sac is opened using a sterile plastic instrument resembling a knitting needle; this procedure, like other types of medical intervention during childbirth, is performed only with the consent of the patient. Amniotomy is safe for the mother and fetus and is absolutely painless.
Lada says that she was very surprised by the absence of medical personnel in the prenatal ward; she imagined that during the entire process of childbirth a doctor or midwife would be constantly next to her. In fact, this is not true: the duties of the maternity ward staff do not include the constant presence of a woman in labor in the room. Normally developing labor does not require constant medical supervision. To provide adequate and timely medical care during childbirth, periodic assessment of the condition of the mother and fetus is sufficient. If the doctor needs to continuously monitor the development, strength and frequency of contractions over a period of time, he can do this using cardiac monitoring - recording contractions and the fetal heartbeat. Periodically entering the room, the doctor studies the recording results and gets a detailed understanding of the development of labor and the condition of the fetus; If there are significant changes in heartbeat or interference in the recording, the device sounds an audible signal to call personnel.
Physicians are required to remain in labor at all times at the end of the second stage of labor - during pushing and birth of the fetus, as well as during the afterbirth period (separation of the placenta). If complications arise before pushing at any stage of labor, the doctor is also constantly on duty at the bedside of the woman in labor. When childbirth proceeds without complications, the doctor should appear in the room at least once every 30-40 minutes, the midwife every 15-20 minutes. Childbirth is a natural process and normally does not require treatment or special actions from staff.
After the amniotomy, the contractions gradually began to intensify, and the midwife advised Lada to get out of bed and move around the ward. The method of behavior that was recommended to our heroine is called active behavior during childbirth. This term refers to the free movement of a woman in labor during contractions and between them, constantly changing positions and moving around the ward, searching for the most comfortable body position.
The movements themselves significantly reduce the overall sensation of pain and help prevent weakness of labor. The level of pain depends on blood circulation. During contractions, the muscle fibers of the uterus contract, wasting energy. The main “energy fuel” for the functioning of all cells in our body is oxygen; myometrial cells (uterine muscles) are no exception. As is known, oxygen is contained in arterial blood; therefore, cell respiration depends on the level and speed of arterial blood flow. When the body is stationary, the overall blood flow decreases, the supply of oxygen to the uterine muscle slows down and pain increases. If a woman in labor walks around the room or moves in a comfortable position, as a result of the movement, the level of blood flow increases and the uterine cells are better supplied with oxygen. Therefore, with active behavior during childbirth, the pain from contractions is much weaker than with a stationary position. During contractions, you should behave freely, choosing the most comfortable body position.
There are many positions that can reduce discomfort during contractions and help you relax. The main principle by which a woman in labor chooses a position during labor is the level of comfort, stability and relaxation. Most birthing poses use four points of support and a predominantly vertical body position; There are also “lying” poses. However, in order for the poses to help, you should change your body position as often as possible and remember to move a little within any pose. Lada found a comfortable position when she stood, resting her hands on the wall and rocking her pelvis from side to side.
As the contractions intensified, Lada was offered to use the shower. The main advantage of aquatherapy is the relaxing and pain-relieving properties of water. In warm water, contractions feel softer, blood circulation improves, the woman in labor has the opportunity to relax and take a comfortable body position, and gets less tired. Water eliminates the occurrence of such side factors of discomfort during childbirth as dry skin, increased sweating, chills or a feeling of heat.
Lada was advised to take a shower at 6 am, but she decided to “delay the pleasure and scheduled a shower for herself at 7 am.” This behavior of a woman in labor is wrong: a woman cannot “manage” her labor herself, make appointments for herself, because she is simply not able to objectively judge the development of the process. Of course, during childbirth it is better to behave freely, actively, to use various non-drug methods of pain relief, however, what and when is the best thing to do, the doctor will advise you more competently. This is very clearly seen in the example of our heroine: having postponed going to the shower for an hour, Lada could barely wait for that hour, she was very tired and exhausted, and as a result, the shower was no longer as effective for her as it could have been at earlier stages. At the same time, if Lada had listened to the midwife and gone to the shower an hour earlier, she would have endured the contractions much easier and saved a lot of energy.
At the end of the first stage of labor, Lada, who had not slept well at night and was exhausted by the precursor contractions, began to get tired; The general fatigue of the woman in labor was also reflected in the development of labor: contractions became shorter and no longer increased, and the dilatation of the cervix did not increase. In order to enhance labor, our heroine was prescribed OXYTOCIN. This drug, used to induce labor, is a complete analogue of the natural hormone oxytocin, released in a woman’s body during childbirth. It is this hormone that is responsible for the development of labor, the natural increase in contractions, dilation of the cervix, the advancement of the fetus through the birth canal and the separation of the placenta (placenta, umbilical cord and membranes) after the birth of the child.
To ensure that the hormone enters the patient’s blood and is absorbed similarly to its natural release in the body, the drug is diluted with saline and injected into the bloodstream very slowly. Drip administration time is 1.5-2 hours. This speed allows you to avoid too violent a reaction from the uterine muscle and completely recreate the picture of the natural regulation of the development of labor.
After the administration of OXYTOCIN, the contractions became noticeably stronger and more painful. To get rid of the pain, Lada tried screaming during the contraction. This decision is wrong - regardless of the reason that prompts a woman in labor to scream, screaming during childbirth is not worth it. Firstly, screaming does not have an analgesic effect, that is, literally screaming does not make you feel better. Secondly, and this is the main thing, screaming during childbirth can harm both the woman in labor and the baby, and also generally negatively affect the course of the birth process. And thirdly, a woman screaming during a contraction scares other women in labor and interferes with the work of the maternity ward staff. If a woman screams during contractions, most of the air she inhales is spent screaming. This means that the fetus, already experiencing hypoxia (lack of oxygen) during contractions, will not receive a sufficient dose of oxygen.
As a result, the condition of the fetus may worsen. The lack of oxygen in the mother's blood, which occurs against the background of screaming, also negatively affects the contractility of the myometrium - the muscles of the uterus. In order for a muscle to contract well, it needs an influx of arterial blood rich in oxygen. The decreased oxygen content in the blood as a result of screaming can lead to the development of weak labor. This complication of childbirth, worsening the condition of the mother and fetus, requires medication and sometimes surgical intervention.
A woman who screams during contractions loses strength and gets tired much faster. If the woman in labor is exhausted, it is difficult to expect normal development of labor.
When it was time to push, Lada was faced with a new problem: instead of straining her stomach and pushing the baby out, she took in full air in her cheeks and “pushed into her face.” Pushing is the tension of the diaphragm and abdominal muscles; it feels similar to the actions of emptying the intestines. Pushing involves a lot of effort, and for it to be effective, you also need to use your breathing correctly. Before pushing, you need to tilt your head back and take a deep breath through your mouth, then hold your breath and press your chin to your chest. Correct inhalation before pushing is similar to inhaling before diving under water: the air should fill the lungs to the limit, and the upper airways should remain free. This inhalation technique in itself encourages abdominal tension; the chest expands, the lungs filled with air force the diaphragm to descend, resulting in increased pressure in the abdominal cavity. By pressing her chin to her chest, the woman in labor groups herself for pushing and protects herself from premature exhalation when the press is tense.
During the examination after giving birth, Lada was found to have a first-degree perineal rupture - this is a minor superficial damage to the skin around the vaginal opening. Lada decided that the gap was formed due to the fact that she tried several times to push without a contraction; this does not actually apply to the causes of perineal trauma. Tears during childbirth are formed due to poor tissue extensibility, inflammatory processes in the vagina, or when the woman in labor tries too hard.
In the first minutes after the completion of labor, Lada felt tired and empty; she did not experience the emotional uplift that her friends described to her. In the first minutes after the birth of a child, many women are in a state of passion - at this moment a large amount of adrenaline and endorphins are simultaneously released in the body of the postpartum woman. Someone cries with happiness, someone laughs, and someone - like our heroine - is in a state of apathy; All these behavior options are associated with unloading the nervous system, relaxing the body after the colossal stress experienced during childbirth. The “chills” that plagued Lada in the first minutes after childbirth are also connected with this - it’s a tremor, multiple relaxation of the motor muscles after overexertion during contractions and pushing.
Procedures for preparing the cervix
If the doctor does not determine that the cervix is high and soft at 38-40 weeks, then this indicates an unreadiness for childbirth. In this case, means are used to accelerate the smoothing of the cervix.
To soften it better, “No-spa” can be prescribed. It has proven itself well, since a decrease in internal tears has been noted when using it. Male sperm also helps soften the cervix, since it contains prostaglandin, which affects the ripening of the cervix. Also, during sex, when a woman reaches orgasm, the muscles of the uterus contract. This helps to launch the birth process.
The doctor may prescribe special gels or vaginal suppositories containing the synthetic hormone prostaglandin. Cheap and effective kelp seaweed sticks are also used. They contain substances that provoke the opening of the internal pharynx, smoothing and softening of the cervix.
Acceleration of cervical dilatation. Non-drug method
If a woman has no contraindications, and the due date has already come to an end, then the obstetrician-gynecologist can advise speeding up this process at home.
The most effective way to speed up labor is sex. Due to the content of prostaglandins in sperm, which stimulate the cervix to open. But despite all the effectiveness of this method, there are a number of contraindications:
- the man has an infection;
- the placenta is quite low;
- too active sex and orgasm.
You should not get too carried away with such an interesting method, so that placental abruption does not occur.
A good way to speed up labor is exercise or exercise. In this case, the process of accelerating disclosure will occur much faster. This could be walking at a slightly faster pace, squats, or walking up flights of stairs. Although doing yoga and going to the pool during pregnancy are necessary physical activities, too much of them can lead to early labor.
You can do household chores: clean the house and wash the floors. But again, do not overdo it so as not to harm the child.
Also, on the advice of a gynecologist, active massage of the nipples will yield results. This process helps to increase the contraction of the uterus, due to which childbirth will not be long in coming. This activity is recommended only for women who have given birth, so that the “afterbirth” leaves the uterus faster. It also helps contract the uterus after childbirth. This process helps to increase the contraction of the uterus, due to which childbirth will not be long in coming.
Taking a warm bath will help speed up the opening process. The water should not be hot! But this method should not be used if the amniotic fluid has broken or the plug has come off.
At home, you can do a cleansing enema or take a small amount of laxative. The effect of the drug will begin within 30 minutes, after which contractions may begin. Castor oil is a laxative in its properties.
There are also several products whose use will lead to rapid dilatation of the cervix. They are raspberry tea, beets, parsley.
The expectant mother can combine some of these tips together. And then the main event in her life will not take long to arrive. But you need to do this only when the period begins to exceed 40 weeks, not in advance.
Methods and tips for accelerating cervical dilatation vary from person to person. For some women in labor, one thing is suitable and works immediately. Some people try all the methods, but the results take a very long time. Therefore, a woman needs to be under constant medical supervision so as not to harm herself or her child.
Perhaps there are women among the readers who have found some other special means to speed up the cervix. Then feel free to share them with your readers in the comments!
Video: Preparing for an easy birth - holding, breathing, dilation of the cervix
PREPARING FOR AN EASY BIRTH: Behavior, breathing, cervical dilatation
Video: the beginning of labor - dilatation of the cervix
Beginning of labor - dilatation of the cervix
Folk remedies
To make the cervix soft, you can resort to folk remedies, but only after consulting a doctor:
- Drink decoctions and infusions of rose hips, hawthorn, raspberry leaves and sage.
- Nipple massage. They need to be gently and gently massaged for 10 minutes 3 times a day. This naturally produces the hormone oxytocin. It promotes contraction of the uterus.
- Evening primrose oil capsules. It is rich in fatty acids, which stimulate the production of prostaglandin. The dosage regimen is prescribed by the doctor.
- Eating fatty fish: mackerel, herring, sprat, silver carp and others.
If during pregnancy the question arises as to why the cervix is soft and what this means, then at the beginning or middle of pregnancy this indicates deviations and the threat of miscarriage. And in the later stages, this is a natural phenomenon that prepares the body for childbirth.
Acceleration of cervical dilatation. Medication method
Childbirth can begin as early as 38 weeks, i.e. If the gynecologist at the appointment discovered a dilatation of 2-3 fingers, then you can prepare for the maternity hospital in advance.
It happens that a woman is simply past her due date (41 weeks of pregnancy), and the cervix has not yet dilated. This can lead to fetal death. Due to the fact that the placenta matures and becomes thinner by its due date, this slows down the supply of nutrients to the baby. For this, doctors use stimulants:
- gels;
- candles;
- droppers;
- pills;
- catheter;
- seaweed;
- folk (home) methods.
There are medicinal and non-medicinal methods to speed up the dilatation of the cervix.
Gels
Photo of the gel
The most gentle means to speed up labor are gels. Its hormonal basis provides acceleration for full disclosure. The composition includes prostaglandin, due to which the processes are accelerated. The effect occurs after 40 minutes and up to 4 hours, it all depends on the individual characteristics of the body.
Gels have been used in obstetrics for about twenty years, which speaks volumes about their work and effectiveness.
The drug is administered with a syringe into the vagina and only as prescribed by a doctor. This is done either by a nurse or by the doctor himself. After which the woman needs to lie down for half an hour to prevent leakage.
The patient is under control and if the gel does not work and the cervix does not open in any way, then it must be reintroduced. During the entire period of use, the gel is administered only in the amount of three milligrams.
If, upon first administration, the cervix is 3 mm, then repeated use is not required. This means that the process of disclosure has already begun to gain momentum.
The doctor prescribes the gel if:
- the cervix does not open in any way;
- contractions are not stable, gradually disappearing;
- there are no contractions at all, even if the amniotic fluid has broken;
- there is a failure at the onset of labor;
With all its positive qualities and gentle properties, the gel also has contraindications for use:
- the mother has individual intolerance;
- poor maternal health;
- the baby's head is larger than the mother's pelvis;
- incorrect presentation of the fetus;
- the child has problems that are diagnosed by a heart monitor.
The doctor must monitor all health indicators of the mother and child, but on what basis should he make a decision on the use of any medications.
Candles
Suppositories also have minimal side effects. This type of medication contains prostaglandins, which help the cervix to open faster.
It is used by inserting a suppository deep into the vagina. The action is carried out by a nurse or doctor. The effect occurs half an hour after application. At the same time, the woman can move around without fear that the candle may fall out.
If the effect does not occur, other methods necessary for delivery are used.
This method only affects the uterus and does not harm the baby. It is used as often as gels.