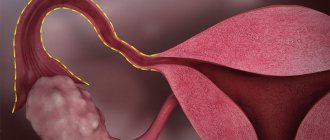
Laparoscopic tubectomy
(salpingectomy) – surgical removal of the fallopian tube using endoscopic equipment. Can be one-sided or two-sided. In women of reproductive age, tubectomy is performed when there are extensive irreversible changes in the organ wall that cannot be eliminated using organ-preserving treatment methods. The main indications for surgery are tubal pregnancy, pyosalpinx and hydrosalpinx. Laparoscopic tubectomy is performed through 3 or 4 punctures in the area of the anterior abdominal wall. It is performed in a hospital setting on a planned or emergency basis under general anesthesia. After a unilateral tubectomy, normal conception is possible; after a bilateral tubectomy, the use of reproductive technologies is necessary.
- Indications and contraindications
- Preparing for a tubectomy
- Methodology
- After tubectomy
- Prices in Moscow
Laparoscopic tubectomy is a relatively simple, minimally invasive surgical procedure. Along with other endoscopic operations, it is widely used in modern gynecology. It has a number of advantages compared to open tubectomy. It allows you to significantly reduce the level of tissue trauma, reduce the risk of infection, reduce the length of hospital stay and the overall rehabilitation period.
Laparoscopic tubectomy belongs to the category of recently emerging surgical methods that successfully compete with traditional operations. Endoscopy in gynecology began to be used at the beginning of the last century, however, due to imperfect equipment, this technique for a long time was primarily of a diagnostic nature. The report on the first successful laparoscopic tubectomy was published by Shapiro in 1973, but the technique began to be used in widespread clinical practice only in 1986, after the advent of technology for transmitting images from the eyepiece of a laparoscope to a monitor screen. Currently, laparoscopic tubectomy is used both in the process of planned treatment of a number of diseases (hydrosalpinx, extensive damage to the tubes as a result of previously suffered pathological processes, etc.), and in the event of emergency conditions (with ectopic pregnancy and pyosalpinx).
Pain after tubectomy and other consequences
Initially, it was believed that this operation did not have any negative consequences. But the fact that the pipes are connected to other organs by one circulatory system can manifest itself in a negative way. The ovaries may become inflamed after a tubectomy. Even after unilateral surgery, signs of disruption throughout the neuroendocrine system may occur. In almost 40% of cases, at least one of the following consequences occurs:
- The appearance of pain in the groin and abdominal area;
- Enlargement of the mammary glands;
- Thyroid gland dysfunction;
- The appearance of hypertrichosis;
- Weight gain.
In addition to all this, common complaints of malaise, headache and increased blood pressure may occur when a right tubectomy has been performed. All manifestations are purely individual and for many the consequences really do not manifest themselves in any way. If a bilateral tubectomy is performed on both sides, the consequences may become more serious.
Consequences of fallopian tube resection
Such an operation disrupts the maturation process of the follicle, causing the reproductive system to suffer. This complicates the process of ovulation - the release of a mature egg from the ovary. The fallopian tube cannot be restored after removal. The main consequence of the operation is a limitation or reduction in the function of childbearing. Surgery to remove the uterine tube causes neuroendocrine disorders. The following symptoms indicate them:
- increased sweating;
- headache;
- pain in the heart area;
- dizziness;
- feeling of heartbeat;
- rushes of blood to the upper body;
- irritability, nervousness;
- thyroid dysfunction.
Judging by the reviews, these symptoms intensify during menstruation. They occur in only 42% of women who have undergone such surgery. Symptoms are observed more often in the early recovery period, while the body adapts to the new condition. With bilateral tubectomy, the risk of such complications is higher. The consequences also apply to the mammary glands:
- In 6% of patients they become rough.
- In 15% of cases, the breasts become larger due to diffuse expansion of the lobules.
Laparotomy, tubectomy: video
In fact, there is nothing terrible in carrying out the operation, since specialists encounter such things very often. When a tubectomy is prescribed, the surgical technique involves a preliminary laparotomy to facilitate access to the internal organs. The cavity incision is then stitched and does not cause any serious consequences.
Even if the operation went well, if sex occurs after a tubectomy, the side of the opposite tubes is pulled. Unilateral surgery leaves a chance to get pregnant naturally. The chances are reduced by 50%, but for a healthy tube there are no contraindications or additional difficulties. If a bilateral tubectomy was prescribed for an ectopic pregnancy, or there was a repeat ectopic pregnancy and the second tube had to be removed, then IVF becomes the only chance to conceive. This is true even with normal ovarian function.
Tubectomy: surgical technique
Tubectomy is a very important operation. It consists of several stages. If a tubectomy is prescribed, the procedure proceeds as follows:
- First, a laparotomy is performed;
- The ovary, from which the damaged tube originates, is freed from adhesions and the problem area is lifted;
- They wrap it on a special leg and add antirheumatic clamps;
- Mark the incision line, which should be above the damaged area;
- Bleeding areas are sutured to avoid complications after surgery;
- The pelvic cavity is examined to ensure that nothing unnecessary remains in it;
- After the bleeding has completely stopped, the abdominal cavity is sutured.
Tubectomy: indications
Surgery is the last resort to solve problems with the fallopian tubes. If the patient is prescribed a tubectomy, the indications for this must also be significant, especially for bilateral surgery. The operation is carried out only with her consent. The main indications for it may be:
- Ectopic pregnancy, when the fertilized egg is already large in size;
- Burst fallopian tube;
- Serious infectious and inflammatory diseases leading to loss of functionality;
- There is a high risk of ectopic pregnancy during conception.
Preparing for a tubectomy
Preparatory processes for this operation may not be carried out at all, with the exception of the administration of painkillers if emergency surgery is required. This happens when an ectopic pregnancy or an infectious disease was detected at a late stage and the woman loses consciousness at this time, a tube ruptures, and so on.
If there is time for preliminary preparation, then a blood test is taken before the operation, painkillers are selected and the period of the cycle is selected when it is best to perform the operation with the fewest possible complications.
Preparation for salpingectomy
Removal of the uterine tubes is carried out under anesthesia, so the woman first undergoes an examination. It includes the following laboratory and instrumental diagnostic methods:
- Fluorography or chest x-ray. This test helps identify signs of tuberculosis or other diseases of the respiratory system.
- Blood analysis. Detects infections, inflammatory processes and diseases of internal organs. For accuracy, blood is taken on an empty stomach.
- Colposcopy. This is a study of the walls of the vagina and cervix, which helps the doctor identify suspicious areas of the mucosa.
- Analysis of urine. For research, a morning portion of urine is given. The study helps evaluate kidney function and identify disturbances in water-salt metabolism.
- Tests for HIV, syphilis, hepatitis. If there is one of these diseases, then doctors take measures to prevent complications. The study is carried out using ELISA.
- Ultrasound of the internal genital organs. It is carried out to assess their condition and select the optimal intervention technique.
- Coagulogram. This is a blood clotting test. Any operation is associated with blood loss, so the doctor needs to assess the risks. Blood for a coagulogram is taken from a vein.
- Electrocardiogram. Necessary for assessing the condition of the heart. This allows us to identify contraindications to surgery, the optimal intervention strategy, dosage and type of anesthesia.
- A smear of the cervix and vaginal mucosa for flora and degree of purity. This test identifies possible genital infections.
The last study is carried out during an examination by a gynecologist. After all the procedures, the woman is sent to a therapist to obtain consent for the operation. Before the procedure, there is a conversation with an anesthesiologist, who determines the optimal option for pain relief and possible risks. Other nuances of preparing for the intervention:
- A woman should notify her doctor about all medications she is taking.
- Anti-inflammatory drugs, anticoagulants and antiagrenants should be discontinued 2 weeks before surgery.
- The evening before the operation, the woman is prescribed cleansing food. You can eat and drink no later than 12 hours before the intervention.
- If there is severe anxiety, the woman is given a sedative at night.
- Immediately before the operation, the woman takes a shower, removes hair from the pubis and perineum, and changes clothes.
Consequences of tubal removal: reviews
Carrying out even the simplest operations on the internal pelvic organs can be unsafe for health. From time to time, the need for emergency operations arises, which further complicates this process. At the same time, if the fallopian tubes were removed, the consequences after this can be much simpler than after treatment. This is due to the fact that the source of the problems goes away and only the consequences caused by the operation, if they occur, remain. The risk of negative consequences depends on the qualifications of the doctor who performed the operation.
Fallopian tubes removed: consequences after surgery
If the fallopian tube is removed, the consequences may manifest itself in bleeding. This is one of the most terrifying phenomena, as the unstoppable flow of blood can cause shock. When removed or torn, the first priority is to bandage the areas that are bleeding. This is harmful not only due to blood loss, but also possible infection of nearby organs. Complications in this case can be caused by the use of vasoconstrictor drugs and other things that affect this process. Even if the tube has not ruptured and is still in a completely normal condition, complications can arise due to non-radical removal of chorion elements. To avoid complications, the surgeon should rinse the tube with saline solution.
The next problem is the appearance of adhesions in the pipe, which have not been removed. After all, this is the same operation on the pelvic organs, albeit on the opposite fallopian tube. There also remains a risk that complications may appear on the second. But this prospect is not so great as to remove the second one at once, since everything can go quite normally. To prevent complications of this kind, Ringer's solution is used, and all blood clots located in the internal cavity are completely removed.
If we consider the removal of the fallopian tube during an ectopic pregnancy, the consequences in their most terrible manifestation for many women are infertility due to the loss of functionality of the second tube.
How to remove the fallopian tube
Resection is performed using one of two methods. The first method is laparotomy. This is an abdominal operation in which a large incision is made on the abdominal wall:
- Longitudinal from the navel to the pubic symphysis. This is a lower midline laparotomy. It can be performed for abundant adhesions, large benign neoplasms of the appendages, malignant tumors, and pelvic peritonitis.
- Transverse, just above the pubis along a fold of skin (according to Pfannenstiel). This incision offers better cosmetic results and faster recovery. This laparotomy is performed when laparoscopy is not possible, but the intervention does not require emergency.
- Longitudinal, just above and just below the navel. This is a midline laparotomy, which is technically simpler and faster than other types of incision. In this way, urgent and emergency operations are performed in case of bleeding, developing peritonitis or rupture of the cystic cavity of the appendages.
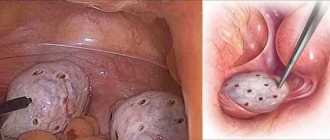
The second way to remove the uterine tube is laparoscopy. With this method, access to organs is achieved using several punctures in the abdominal wall. The surgeon controls his actions using images on the monitor. It is obtained through a microvideo camera, which is inserted together with instruments into the abdominal cavity.
If a woman does not have indications for emergency surgery (intra-abdominal bleeding, etc.), then resection of the fallopian tube is often performed laparoscopically. The advantages of this method compared to laparotomy:
- less traumatic;
- only small incisions remain (up to 1.5 cm);
- less severe and less lengthy rehabilitation.
Laparoscopy
The cost of such an operation varies between 30-50 thousand rubles. Laparoscopy does not last long - about 40 minutes. After the operation, the woman regains consciousness within 1-2 hours. The favorable time for laparoscopy is the 7-10th day of the menstrual cycle.
With this operation, both endotracheal combined anesthesia and epidural anesthesia are possible. Laparoscopy technique:
- Several incisions are made in the abdominal wall: near the navel, above the pubis and in the lower abdomen.
- Trocars are installed in them, through which the necessary instruments are inserted. A Veress needle is inserted into one, which creates pneumoperitoneum - inflation of the abdominal cavity by injecting carbon dioxide or oxygen for a better view.
- An endoscope and other laparoscopic instruments are inserted into the remaining holes.
- After the blood is suctioned, the patient's pelvis is elevated 45 degrees to create the optimal position for pelvic surgery.
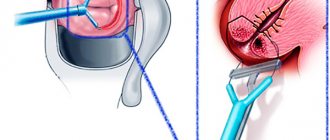
- The doctor finds the tube to be removed, clamps it as close as possible to the cut-off site and pulls it tight.
- The appendage is cut off using forceps, laparoscopic scissors or a bipolar coagulator.
- The bleeding vessels are coagulated and the upper part of the broad uterine ligament and the isthmus of the tube are cut off.
- The severed appendage is removed through the largest trocar to the outside.
- Sutures are placed on the trocar holes, and sterile drapes are placed on the wounds.
Laparotomy
Abdominal surgery is always performed under general anesthesia, so it lasts at least 1.5 hours. The cost of laparotomy tubectomy ranges from 10 to 20 thousand rubles. depending on the complexity of each case. General procedure for the operation:
- After induction of anesthesia, the doctor performs a Pfannenstiel or other incision, depending on the indications for which the intervention is performed.
- Blood that has entered the abdominal cavity is pumped out and collected in vials so that it can be transfused in the future.
- The tubes and the uterus itself are removed to find the source of the bleeding.
- A clamp is applied to the isthmic portion of the appendage and mesentery.
- The appendage is cut off, the peritoneum is sanitized and the dissected tissue is sutured.
Bilateral tubectomy: consequences
If we consider the consequences of removal of the fallopian tubes, reviews from many patients indicate that the first few months after the operation, painful sensations still make themselves felt. Consequences of this kind manifest themselves in each case individually, but you should be prepared that several cycles may occur problematically. Feelings during menstruation may also be more painful, and the cycle itself may be greatly disrupted. These manifestations are typical only in the first months. If they bother you for more than six months, then you should consult a doctor.
Recovery after tubectomy
When performing an operation using laparoscopy, a woman can go home within a couple of days. After laparotomy, she is in the hospital for 10-14 days until the stitches are removed. Already in the first days, recovery includes early activation. This helps reduce the risk of thrombosis, intestinal paresis and pain. Measures to prevent adhesions:
- Introduction of barrier absorbable gels into the abdominal cavity before completion of the operation.
- Get out of bed the very next day after the procedure. Walking calmly helps minimize the risk of adhesions.
- Carrying out electrophoresis with zinc and iodine.
According to indications, doctors prescribe antibiotics and analgesics to the woman. On the first day, the patient is offered light soup, cereals and drinks, then fermented milk products and lean meat are introduced into the diet. You need to exclude foods with fiber from your diet, as they provoke increased gas formation.
After removal of the tubes, the ovaries continue to produce eggs, the uterus also prepares to receive the embryo, i.e., the main functions are preserved. If one tube is preserved, the woman can become pregnant. Rules for late recovery after tubectomy:
- Sexual activity can begin no earlier than a month after surgery and if you are in good health.
- Before the sutures are removed, they are kept clean and dry. Instead of a bath, they take a shower, covering the wounds from getting wet with a bandage.
- Limit sports and intense physical activity for a month. Sometimes a woman is recommended to wear a bandage during this period.
- For six months after removal of one or both fallopian tubes, you should not lift heavy objects.
- A woman must take birth control for 6 months to prevent pregnancy.
Resumption of the menstrual cycle
Recovery occurs individually for each woman. Most often, menstrual irregularities are temporary. It can be restored with hormonal correction. Normal cycles often alternate with disrupted ones. Features of menstruation restoration:
- If the body quickly adapts or a hormonal imbalance occurs, then menstruation may begin within a couple of days after the operation. The first cycle will be longer than all previous ones.
- Early onset of menstruation after tubectomy is rare. For most women, it comes on time.
- In other patients, recovery of the cycle takes about 2 months. This is not considered a deviation. If the cycle has not returned to normal after 60 days, then you need to consult a doctor, as there is a risk of endocrine disorders.
Fallopian tube removal, laparoscopy, consequences, reviews
Laparoscopy has become one of the main operations for treatment. This is quite justified, since it is a relatively simple, affordable and safe technology. It is used for many types of treatment of the pelvic organs, as well as for their diagnosis.
Reviews about this procedure are much more positive than about other treatment methods. Removal of tubes using a laparoscope is carried out with maximum precision, which minimizes the risk of negative consequences that should be feared.
Pregnancy after right tubectomy
When only one tube was promptly removed, pregnancy is quite possible. There are several conditions for this, but when the right pipe is removed, as a rule, the left one remains and functions quite normally. This also applies to the removal of one left pipe, when the right one remains normal.
If complications arise, it is possible that the second remaining pipe has become obstructed. This means that the risk of an ectopic pregnancy in it increases significantly, not to mention those cases when adhesions make the cavity completely impassable. A tubectomy for an ectopic pregnancy is the most common solution, so if the situation recurs, you can lose both tubes.
Eco after tubal tubectomy
If an operation was performed to remove both fallopian tubes, regardless of whether they were removed at the same time or after some time, the woman becomes infertile. Natural conception in this case is impossible. This does not depend on age and other factors. But experts suggest IVF in this case. Removal of the fallopian tubes does not affect the functioning of the ovaries in any way, unless complications arise. The egg matures normally, but cannot move into the uterus and meet sperm.
IVF without fallopian tubes is quite normal. Their absence even protects against complications that may arise in the presence of a pipe. There are no contraindications for artificial insemination in the absence of tubes. The supervision of doctors will help to carry the fetus normally and without complications. The main thing here is to withstand a certain period of several cycles so that fertilization takes place in a state favorable to the body. If the uterus was not damaged, then the fetus will be able to latch on well. When using a protocol with three embryos simultaneously implanted in the uterus, the probability of pregnancy is more than 50%.
Complications of salpingectomy
A separate group includes the effects of anesthesia. They go away on their own within a few hours or days. The list of such complications includes:
- vomiting;
- chills;
- nausea;
- weakness;
- sore throat (due to intubation with a tube);
- dizziness;
- pain in the area of the postoperative wound.
The other group consists of the consequences of the operation itself. After a tubectomy, a woman may develop the following complications:
- Hematomas in the peritoneal cavity or thicker subcutaneous fat. They can provoke bleeding. This indicates problems with the blood clotting system or that the surgeon performed hemostasis poorly.
- Inflammation. This is indicated by a temperature that rises immediately or a couple of days after the operation.
- Adhesions that disrupt the functioning of internal organs. They can occur both after laparotomy and after laparoscopy.
- Bloody vaginal discharge. Most often minor, they occur after surgery to remove a pipe due to its rupture. Bloody discharge is not considered a serious complication because it is caused by blood being pushed into the uterus during surgery.
- Ectopic pregnancy. If it was the reason for the removal of one of the tubes, then there is a high risk of its development in the remaining appendage.
Articles on the topic
- Uterine bleeding - causes and surgical treatment
- Consequences of endometriosis in women - risk of developing cancer and other pathologies
- Consequences after tubal laparoscopy and how to avoid them
Laparotomy tubectomy method
Laparoscopy is an operation that is performed using endoscopic equipment. It is prescribed if all of the above conditions are absent. During the procedure, the abdominal anterior wall is punctured with a Veress needle. Then a special gas is injected under pressure into the peritoneal cavity. A manipulator and an endoscope are used during laparoscopy, for which trocar tubes are inserted. A video camera allows you to magnify organs by displaying the image on a special monitor. This operation is the least traumatic and has a minimal recovery period.
This method of surgical intervention involves an incision in the abdominal anterior wall to access the uterus and appendages. The incision can be either inferomedian (from the navel along the midline) or transverse (two to three centimeters higher from the symphysis pubis).
An inferior midline incision is a simpler method of performing laparotomy, but is more traumatic. It is used primarily if there is an urgent need to stop severe bleeding. In addition, this method is used in the presence of tumors (tubo-ovarian, malignant), adhesions that have spread to large areas of internal organs, and pelvioperitonitis.
The transverse incision is not so traumatic, used in the same, but not in such emergency cases and subject to a smaller volume of surgical intervention. After it, the body recovers faster. This method also involves applying a cosmetic suture.
All types of tubectomy are performed using combined general endotracheal anesthesia. The fallopian tube (its uterine region, as well as the mesentery), which needs to be removed, is clamped with special clamps. In this case, the bleeding (if present) stops, after which the fallopian tube is directly removed over the clamps. If there is an adhesive process, the adhesions must first be cut.
Planning a pregnancy
The possibility of conceiving a child depends on the type of tubectomy performed. If only one fallopian tube was removed, then if it is functioning normally, pregnancy is possible, but the chances are reduced by at least 50%. The likelihood is even lower if the remaining appendage is changed, inflamed or has adhesions. If a woman does not have one fallopian tube, then the following options are possible:
- Ovulation does not occur, the follicles begin their reverse development. More often this occurs due to hormonal imbalance.
- The egg is released into the abdominal cavity. Since it is not captured by the fimbriae of the tubes, after 2 days it dies and is destroyed.
- The egg floats in the abdominal cavity and reaches a healthy tube, through which it passes into the uterus. It will be easier to capture the follicle if it is released from the ovary from the side of the preserved epididymis.
The probability of getting pregnant on your own with one fallopian tube is on average 56-61%. Doctors advise planning to conceive after six months, others recommend waiting 1-2 years. During this time, it is possible to normalize the functioning of the neuroendocrine system. Only then will the woman’s body be ready to bear a child.
If both fallopian tubes were removed, then either the egg constantly dies in the peritoneal cavity, or the ovaries undergo reverse development. In this case, you can only get pregnant through in vitro fertilization (IVF). This procedure can be resorted to after 6-12 months.