Infiltrative breast cancer develops from degenerated epithelial cells of the tissues of the lobules or ducts of the organ. The primary form of cancer occurs more often after 40 years of age, and the secondary form develops at any age. Infiltrative breast cancer is an aggressive form of the disease, prone to rapid metastasis. Atypical cells spread through the blood and lymph. They affect lymph nodes, muscles, joints, kidneys, liver, bones, and lungs. Often latent tumor metastases do not manifest themselves for a long time. Tumor recurrence can occur many years after treatment.
The Yusupov Hospital sees a mammologist and an oncologist. The hospital's oncology clinic is equipped with modern diagnostic equipment that effectively detects malignant and benign tumors at an early stage of development. The appearance of the first symptoms of discomfort: pain in the mammary glands, lumps in the glands, changes in the color of the skin of the breast - this is a reason to contact an oncologist. After the examination, the doctor will select the most effective treatment for this form of cancer. The hospital treats cancer using modern techniques, using radiation therapy, targeted chemotherapy, and hormonal therapy. As a result, the quality of life of a woman improves and her life expectancy increases.
Causes
Currently, there is no reliable information about why infiltrative breast cancer begins to develop. Scientists are of the opinion that the growth of a malignant tumor can begin under the influence of many provoking factors:
- Hereditary predisposition - the tumor develops more often in women whose immediate female relatives had breast cancer;
- Increased sensitivity of receptors to progesterone or estrogens, which are located in breast tissue, are involved in the synthesis of proteins and messenger RNA, and the release of cytokines. As studies have shown, they can also be involved in the mechanism of formation and development of a malignant breast tumor, the development of metastases;
- Hormonal imbalance in a woman’s body;
- Age – women over 40 years of age are more likely to get breast cancer;
- Late menopause;
- Obesity.
The risk of developing infiltrative breast cancer increases in women who have not given birth, have had frequent abortions, have undergone long-term therapy with hormonal drugs, and have been exposed to radiation. Factors that can trigger the formation of a malignant tumor in the mammary gland include early puberty, alcoholism, and drug use.
What could be the complications and consequences?
The presence of infiltrative cancer can result in some serious complications:
- Rapid metastasis of the tumor to the lymph nodes and various organs. The disease can affect the lungs, musculoskeletal system, liver, brain, adrenal glands, and appendages.
- Loss of motor ability of the upper limb in the area of the shoulder on the side where the cancer formed.
- Lymphostasis of the hand.
- Relapse of the disease 5-10 years after treatment.
If there is no treatment for a long time, the oncological process will spread to tissues and organs located both nearby and at a distant distance. The longer the start of therapy is delayed, the higher the risk of death.
Kinds
There are the following degrees of differentiation of tumor cells in infiltrative breast cancer:
- Gx – it is not possible to determine the degree of differentiation;
- G1 – highly differentiated malignant tumor;
- G2 – moderately differentiated neoplasm;
- G3 is a poorly differentiated malignant tumor.
- G4 – undifferentiated malignant process.
There are several types of infiltrative breast cancer:
- Infiltrative lobular;
- Edema-infiltrative;
- Ductal;
- Infiltrative nonspecific type.
Infiltrative lobular cancer is found in the upper part of the breast in older women.
It occurs in 10% of cases of infiltrating breast cancer. Oncologists distinguish two types of edematous-infiltrative breast cancer: primary (diffuse) and secondary (nodular). Infiltrative ductal breast cancer affects most older women. The diagnosis of “infiltrative nonspecific breast cancer” is established when the differentiation of neoplasm cells is difficult. The following nonspecific forms of infiltrative cancer are distinguished: mucinous cancer, squamous metaplasia, poorly differentiated tumors.
Make an appointment
Types and stages
To draw up a treatment or surgical plan, it is important to know exactly the type of carcinoma. First of all, the degree of neglect of the pathology is determined (the more severe the stage, the more aggressive treatment is required). Depending on the extent of the damage to the breast, breast cancer comes in five stages.
- Stage zero (microinvasive cancer, Tlmic): tumor is less than 10 mm, external symptoms are subtle, the patient often does not pay attention to them.
- First stage (T1): the tumor reaches 10–25 mm, and begins to grow (infiltrate) deep into healthy breast tissue.
- Second stage (T2): the neoplasm has a diameter of 25–50 mm. The ingrowth is deep (the boundaries between healthy and diseased tissues are unclear).
- Stage three (T3): tumor larger than 50 mm. Metastasis begins.
The last stage of T4 is no longer measured by the size of the infiltrating tumor, but by its effect on other parts of the patient’s body. In the most advanced form, cancers spread to the chest wall, breast skin, and affect the intercostal muscles and serratus anterior muscle. Metastatic lesions progress beyond the breast. With carcinoma, metastases most often occur in the lymph nodes, bones, liver, lungs, and ovaries.
Edema-infiltrative form
This type of carcinoma is quite rare (6% of all breast cancer cases), but the most difficult to treat. It is not primary. It is always preceded by long-term ductal breast cancer. The peculiarity of the pathology is that the tumor node is difficult to differentiate, which complicates the treatment process: healthy tissues try to fight the tumor with the help of severe inflammation, which “hides” the tumor.
The edematous type of carcinoma is an aggressive form of cancer. In 90% of cases, the “invasion” of the entire mammary gland and the onset of metastases begin within one year after the development of the first stage of the disease. The prognosis for remission is unfavorable.
Infiltrating ductal carcinoma
This is the most common type of malignant lesion of the mammary glands (detected in 72% of cases, mainly among women after menopause). Ductal carcinoma originates in the epithelium of the milk ducts, and then quickly deepens towards the chest, causing necrosis of healthy tissue. The tumor has an uneven shape with sharp edges. With this form, there are no signs of invasion of the basement membrane of the duct, parenchyma and lymphatic system, and metastasis is excluded.
Ductal carcinoma is often a precancer, that is, it remains in the zero stage for a long time. But upon transition to more severe stages it acquires rapidly progressive forms (for example, edematous-infiltrative).
Infiltrative lobular cancer
Lobular carcinoma (lobular carcinoma) is a collection of cancer cells inside the lobules of the breast. Unlike ductal tumors, which are typical for women over 50 years of age, this type of pathology is more common in women under 40 years of age (nulliparous, taking hormones, etc.).
Invasive lobular carcinoma is not detected by mammography. It is detected by palpation (when a lump is detected in the upper outer quadrant of the mammary gland - from the nipple to the armpit), and its malignant nature is confirmed by a biopsy. In 70% of cases, the tumor is single in nature (that is, single-focal, located only in one breast). In other cases, multifocal cancer is detected - tumor nodules are concentrated in the area of one gland or two breasts are affected at once.
Nonspecific infiltrative cancer
This is the name for malignant tumors, the type of which cannot be determined during diagnosis. It is difficult to treat nonspecific breast cancer, since you have to select all methods, focusing on those that cause improvement in the patient.
Nonspecific carcinomas come in four types. The division is based on the degree of damage to healthy tissue by the neoplasm and the rate of division of cancer cells:
- G1 is a poorly visible tumor with a slow development rate.
- G2 is a poorly visible tumor with an average rate of cell division.
- G3 – almost indistinguishable tumor boundaries with a rapid progression.
- G4 – almost indistinguishable tumor with aggressive development.
Nonspecific carcinoma G1 and G2 is difficult to diagnose in the first stages, but if it can be identified, the prognosis for treatment is generally satisfactory. Forms G3 and G4 are difficult to treat, so the prognosis for patient survival is poor.
Symptoms
In most cases, infiltrative breast cancer is almost asymptomatic.
Breast masses are detected by mammologists during a routine examination. Infiltrative lobular breast cancer develops in the lobes of the mammary gland. The tumor is dense, painless, and has uneven contours. Then the skin over the tumor wrinkles and the nipple retracts. Metastases are found in the ovaries and uterus. The nonspecific type of infiltrative breast cancer has several degrees. They depend on the location and number of affected lymph nodes. If 1-3 lymph nodes in the peri-sternal or axillary region are affected, oncologists determine the first degree of development of a malignant neoplasm. If atypical cells are detected in more than four lymph nodes in the axillary region or chest cavity, this is the second degree of cancer development. If more than ten lymph nodes of the axillary and subclavian region are affected, doctors talk about the third degree of tumor spread.
The edematous-infiltrative form of cancer is characterized by swelling of the skin and the appearance of infiltrates - malignant formations. The primary form of the disease is rare. Doctors mistake it for mastitis (inflammation of the mammary gland), since there are no tumor nodes. This type of cancer develops slowly and is latent.
Infiltrative ductal cancer (carcinoma) of the breast develops from the epithelial cells of the milk duct. It is characterized by a large number of morphological structures. The cancerous node has an uneven outline. It fuses with surrounding tissues. Areas of necrosis appear inside the node, cysts form, and microcalcifications are detected. When palpating the mammary gland, a dense node is detected. The skin over it may be red. The appearance of the mammary gland changes. Its volume and shape change, the skin becomes “marbled”.
With infiltrating ductal breast cancer of the first degree, the tumor size does not exceed two centimeters. Metastases in other organs and tissues are not detected. Infiltrative ductal breast cancer of the second degree is characterized by the presence of a node, the diameter of which varies from 2 to 5 centimeters. The tumor can develop without metastases or metastasize to the lymph nodes. In the final stages of development of an infiltrative tumor, bloody discharge may appear from the nipples.
Treatment methods for infiltrative cancer
Infiltrating breast carcinoma is difficult to treat. Therapy is prescribed after undergoing the necessary diagnostic procedures. Therapeutic methods are carried out independently or in a complex form and with the use of auxiliary techniques. The duration of inpatient therapy is 2-3 weeks. A woman will be able to return to her usual lifestyle and go to work 6 months after the end of treatment, in the absence of secondary cancers and complications.
Chemotherapy and medications
Chemotherapy is necessary to treat infiltrative breast cancer. The method is characterized by high efficiency in the treatment of oncological pathologies. The therapy affects the affected areas and affects nearby healthy tissue. The procedure is difficult and is accompanied by multiple adverse reactions - baldness, hair loss, sudden loss of body weight, fatigue and a weakened immune system. Indications for chemotherapy:
- tumor size is more than 20 mm;
- stage 2 cancer;
- woman under 35 years of age;
- a malignant cancerous growth not associated with hormonal imbalance.
Medications push the body to fight atypical tissues. Antimetabolites act on the genetic cellular structure, destroying it during separation - Gemcitabine. Anthracyclines produce free radicals that damage DNA cells - Doxorubicin and Daunomycin. Taxanes - Paclitaxel - act on the progression of affected tissues.
Vinca alkaloids destroy the structure of the atypical cell, provoking further tissue death. The drug has a milder effect - Vinblastine and Vincristine. Targeted treatment is prescribed to women when the tumor develops to a specific gene (triple negative cancer). The therapy uses Trastuzumab, which blocks the intensity of the affected cells.
Surgical intervention
Breast cancer surgery is performed in the following ways:
- Radical mastectomy – preserves muscle structure. Doctors then restore breast shape through surgery.
- Mastectomy with preservation of the areola is performed in the presence of a streaming type of infiltrative cancer. During the procedure, the surgeon removes the tumor and, if necessary, lymph nodes. After the operation, the visual appearance of the breast and the functionality of the organ are preserved.
- Organ-sparing therapy - the tumor is excised without affecting healthy materials. With a small size of the formation and a voluminous mammary gland, the prognosis improves.
- Radical resection is the complete removal of an organ. The operation is performed when the growth is large.
Homeopathy
Homeopathic remedies are used by medical professionals to improve the effectiveness of the rehabilitation period in women after surgery. Homeopathy has proven itself to prevent the development of relapses, to increase and strengthen the immune system of the female body. For treatment, the following drugs are prescribed, taken orally:
- Galium-Hel;
- Psorhinochel;
- Lymphomyosot;
- Phosphorus Homaccord.
Medicines are taken 10 drops in 6 approaches per day. After two months, the woman reduces her intake to 10 drops in 4 approaches per day. After a new 60 days, it is enough to take 3 times a day. As additional measures, the doctor may prescribe injections of the drugs Nux vomica-Gomaccord, Hepel, Berberis-Gomaccord and Chelidonium-Gomaccord. Medicines help remove harmful toxins from the body.
ethnoscience
Traditional medicine is used in cases where there are no results from traditional treatment and when it is necessary to enhance the effectiveness of the functioning of the therapeutic methods used. Non-traditional methods of therapy are a good adjuvant. Traditional treatment recipes involve the use of herbs and plants containing toxic components. Therefore, it is important to strictly adhere to the prescribed permissible dosage in order to avoid deterioration of the body’s condition. You can't focus on just one remedy. It is recommended to combine different tinctures and decoctions.
- Decoction of potato flowers. Take one tablespoon of dried flowers and pour 0.5 liters of boiling water. The mixture is left to infuse in a thermos for 2-3 hours. Then the tincture is passed through cheesecloth and squeezed out. It is recommended to store the resulting broth in a glass container in the refrigerator. Take 160 ml 3 times a day 30 minutes before meals. The duration of the course is two weeks. Reception can be resumed after a 7-day break. The general course of treatment is 6 months.
- Birch mushroom tincture. Grate the mushroom and leave for 2 days in warm water in a ratio of 1:5 mushroom and water, respectively. After 2 days, filter the broth and consume 3 times a day 30 minutes before meals. Store the tincture in the refrigerator for no more than 4 days.
- Decoction of golden mustache. Mix 30 ml of the mixture with 40 ml of unfiltered sunflower oil and drink in one gulp. Repeat the procedure 3 times a day 20 minutes before meals. The course lasts 10 days after 5, then 10 after 10 for 3 months.
Before starting to use traditional medicine, you should consult your doctor. If during the process the patient feels worse, the treatment is stopped and sent for examination.
Complications
Infiltrative ductal tumor of the mammary gland quickly spreads to the skin of the affected breast, nearby tissues, and lymph nodes.
In the ductal form of a malignant tumor, the skin over the tumor, the fatty layer of the axillary region, lymph nodes, and surrounding tissues are involved in the pathological process. Atypical cells migrate to muscles and bones. Metastases spread to the liver, lungs, kidneys, adrenal glands, and brain. When the lymph nodes in the axillary region on the side of the tumor are affected, the outflow of lymph from the vessels of the upper extremities to the main lymphatic collectors is disrupted, lymphostasis develops, and the motor ability of the arm is impaired. Often, several years after treatment, relapses of infiltrative breast cancer occur.
Stages
There are five stages in the development of cancer.
Zero (0) stage
means that the tumor is located where it formed (in the lobule, milk duct). Its dimensions do not exceed 10 mm, there is no germination into surrounding tissues.
Stage 1
corresponds to tumor sizes of 10 - 25 mm. There are no metastases in the lymph nodes or a small (up to 2 mm) single metastasis in the lymph node is possible, but invasion has already begun.
At stage 2
In infiltrative cancer, the tumor grows into the surrounding tissues, its size increases to 5 cm. Or the size remains within 2 cm, but there are metastases in the regional lymph nodes.
At stage 3
the size of the tumor exceeds 5 cm, there are metastases, germination into surrounding tissues (invasion), skin symptoms. At this stage, up to 10 regional lymph nodes are affected.
Infiltrative breast cancer stage 3 is the last stage at which surgical treatment is still possible.
At stage 4
The size of the tumor no longer matters. The main symptom is the presence of distant metastases (in the liver, lungs, brain, adrenal glands, ovaries, uterus, kidneys, bones), as well as tumor growth into the chest wall, muscles (intercostal, serratus), and skin.
Stages of breast cancer November 21, 20201847 2
Diagnostics
At the Yusupov Hospital, early diagnosis of breast cancer is carried out using modern instrumental methods: ultrasound, mammography (examination using X-rays). Also, if a malignant tumor is suspected, oncologists perform the following diagnostic procedures:
- Light scanning - during the examination, infrared light is passed through the breast tissue;
- Thermography - measure the temperature of the breast using an infrared scanner, which allows you to determine the development of the pathological process;
- Ductography - the method is used in the presence of discharge from the nipple; a contrast agent is injected into the milk ducts and radiography is performed;
- Biopsies - using a puncture or scalpel, samples of tumor cells and tissues are obtained, which are sent for cytological and histological examination;
- Pneumocystography - in the presence of cystic formations, a gas mixture is injected into them and an X-ray is taken.
Doctors at the Yusupov Hospital conduct instrumental studies using the latest equipment from the world's leading manufacturers.
Surgeons are fluent in all types of biopsies. Histologists have extensive experience in identifying breast tumors. Laboratory technicians determine the level of tumor markers. Its increase may indicate the presence of a cancer process. Make an appointment
Modern diagnostic methods
To identify a malignant tumor, they resort to the use of effective diagnostic techniques. Initially, anamnesis is collected, in particular, to determine the presence of a hereditary factor. Next, the doctor examines the mammary glands and palpates the lymph nodes.
Making an accurate diagnosis is impossible without instrumental methods:
| Diagnostic type | Description |
| Mammography | Pictures are taken in two positions. The examination allows you to detect compactions, the size of which ranges from 0.5 cm. |
| Galactography | It is carried out when a secretion appears from the chest. |
| Ultrasound of the gland | The technique is appropriate for single education. Helps determine the malignancy of the tumor. |
| MRI with contrast | Used in cases where it is necessary to detect relapses. |
| Thermography | Research is rarely used. Determines areas of increased temperature at the site of tumor formation. |
In addition, tissue samples are taken from the patient for biopsy. You will also need to undergo a general analysis, test for tumor markers and hormone levels. If necessary, chest X-ray, CT and scintigraphy are performed.
Treatment
If a mass formation is detected in the mammary gland, the mammologist at the Yusupov Hospital conducts a comprehensive examination of the patient.
The doctor makes the decision on the treatment method after analyzing the results of all studies. Therapy for infiltrative breast cancer consists of several methods. They are used depending on the type and stage of tumor development, the age and general condition of the patient, and the presence of concomitant pathology. Surgeons at the Oncology Clinic take an individual approach to choosing the method of surgical intervention. Oncologists at the Yusupov Hospital prefer minimally invasive operations, after which the mammary gland is preserved. The breast is removed when other methods cannot save the patient's life. Before and after surgery, hormonal, radiation and chemotherapy are carried out.
Risk factors
The nature of the appearance of G2 cancer is not completely known to science; several theories have been developed to explain the reasons for the formation of cancer cells. Most oncologists agree that cellular damage accumulates in human life, and as a result, the cell's DNA undergoes mutation. Such phenomena are associated with the functioning of the immune and endocrine systems. Excess estradiol leads to negative changes in cells exposed to carcinogens.
The exact mechanism of the disease has not yet been established, but the main risk factors are well known.
- Age over 50
- The woman did not give birth, or she had children after 30 years.
- Late menopause.
- Family predisposition: cases of ovarian or breast cancer in relatives in the direct ascending line (mother or grandmother).
- Atypical tissue hyperplasia (based on biopsy results).
- Excess weight and poor diet, especially excess animal fats.
- Mutated BRCA genes, especially common in representatives of certain nationalities.
The above factors indicate a high risk of developing tumor processes in the body.
Important! The presence of one or more of these factors in a woman does not always lead to the development of cancer. The opposite statement is also true: if a girl has no risk factors, this does not guarantee that she will never develop cancer.
Prevention
Prevention of breast cancer lies in a woman’s attentive attitude to her health.
Oncologists recommend that every woman conduct a breast self-examination every month during menstruation. If you detect the slightest changes in the shape, size, symmetry of the breast, breast skin, areas of compaction or discharge from the mammary gland, immediately make an appointment with a mammologist at the Yusupov Hospital. The doctor will conduct an examination and, if a malignant neoplasm is suspected, arrange a consultation with an oncologist. Women should undergo regular medical examinations and undergo a blood test for tumor markers once a year in the following cases:
- The first menstruation occurred at the age of 11-12 years;
- Menopause came after fifty-five years;
- The woman has never given birth or her first birth was after 35 years of age;
- Burdened by heredity;
- Tumors of a different location were previously identified;
- There is a disease of the endocrine system.
To undergo a comprehensive examination, make an appointment with a mammologist at the Yusupov Hospital.
Call the contact center phone number. Its specialists will select a time convenient for you to consult with a leading specialist in the field of diagnosis and treatment of malignant neoplasms of the breast. The prognosis for life and recovery when infiltrative breast cancer is detected improves with timely initiation and adequate therapy. Make an appointment
Forecast and prevention of the disease
The likelihood of remission and its duration depend on the stage and form of the disease. With edematous infiltrating carcinoma, the prognosis is the most unfavorable. Stages 1–2 of ductal breast cancer are the easiest to treat. According to statistics, after a full course of treatment, patients lived for more than 5 years without relapse:
- Stage 1 – in 75% of cases.
- Stage 2 – in 43% of cases.
- Stage 3 – in 13% of cases.
- Stage 4 – less than 5% of cases.
To increase the chances of survival, it is recommended to conduct courses of targeted therapy after the main course of treatment. The drugs will need to be taken 10–12 times a year throughout your life. The downside is the price of such prevention (purchase of drugs for a year will cost at least 850 thousand rubles), but in 85% of cases they increase survival by 3-4 times (even in late stages with metastases)
Considering that breast cancer is a disease for which all women are at risk, the main thing is to detect the disease in time. All women are recommended to undergo examinations by a mammologist 1-2 times a year, even if there are no symptoms. If you experience pain in the mammary glands, lumps in the chest or armpit, it is important to immediately consult a doctor and undergo a full diagnosis.
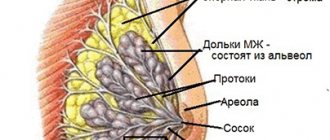
Features of the disease
Infiltrate is a part of tissue consisting of atypical cells of increased size with the ability to rapidly divide. With high-density accumulations, tumors form, growing into adjacent healthy tissues and destroying them. With infiltrative growth, the boundaries of the cancerous formation cannot be clearly defined, and a limited capsule is not formed.
Severe symptoms of infiltrative cancer begin to appear only from the 2nd–3rd stage. At first, symptoms may be confused with other breast diseases and the necessary treatment may not be initiated. Many women do not pay attention to minor chest pains and general weakness, hoping that this is a harmless reaction to stress, approaching menstruation, etc. When a cancerous tumor grows, the following occur:
- Seals in the mammary gland of different sizes and shapes.
- Enlargement of the gland (one breast can become 2-3 times larger than the other).
- Change in skin color. Due to the compression of blood vessels by the tumor and disruption of tissue nutrition, the breast turns red or purple.
- Structural changes in the skin. There may be slight flaking or scabs that make the surface of the gland look like the peel of a lemon.
- The pain becomes constant, worsening when pressing on the chest.
- Abnormal discharge from the nipples (mucus with purulent and bloody impurities).
In the later stages of infiltrative cancer, the patient experiences rapid weight loss. General health worsens, which is expressed in increased weakness, constant nausea, vomiting, and dizziness.
Forecasts
Hormone-dependent carcinomas have a better prognosis if detected early; for example, with stage 1 lobular cancer, the vast majority of women are cured; with stage 2, eight out of ten who received radical treatment live long. The prognosis for stage 3 is sad for half.
When cancer is no longer a fear from your dreams, but a reality and your present with the future, it is important to search for a good clinic, where they know the problem to the smallest detail and have everything for optimal diagnosis and proper treatment. There are such clinics in Russia, and ours is the best representative of private oncology care.
| More information about breast cancer treatment at the European Clinic: | |
| Surgeons-oncologists-mammologists | from 5100 rub. |
| Removal of a breast tumor | from 92,000 rub. |
| Emergency oncology care | from 11000 rub. |
| Chemotherapy appointment | 6900 rub. |
Book a consultation 24 hours a day
+7+7+78
Bibliography:
- Semiglazov V.V./Carcinoma in situ of the mammary gland - morphological and clinical problems// Pract. oncology; 2002; No. 1; v.3.
- Semiglazova V.F., Semiglazov V.V., Manikhas A.G. Breast cancer. Chemotherapy and targeted therapy//-M.: Medpress-inform; 2012
- Hussain M., Cunnick GH / Management of lobular carcinoma in-situ and atypical lobular hyperplasia of the breast—a review // Eur. J. Surg. Oncol.; 2011 Apr; 37(4).
- Litière S., Werutsky G., Fentiman IS, et al./ Breast conserving therapy versus mastectomy for stage I-II breast cancer: 20 year follow-up of the EORTC 10801 phase 3 randomized trial // Lancet Oncol.; 2012 Apr; 13(4).
- Louis-Sylvestre C., Clough KB, Falcou MC., et al. /A randomized trial comparing axillary dissection and axillary radiotherapy for early breast cancer: 15 year results// Breast Cancer Research Treat. Special Issue: 24th Annual San Antonio Breast Cancer Symposium; 2001; 69.