Manual examination of the uterus after childbirth
Retention of parts of the placenta in the uterus is a serious complication of childbirth. Its consequence is bleeding, which occurs soon after the birth of the placenta or at a later date. Bleeding can be severe, threatening the life of the postpartum mother.
Retained pieces of the placenta also contribute to the development of septic postpartum diseases. In case of hypotonic bleeding, this operation is aimed at stopping the bleeding.
In a clinical setting, before surgery, inform the patient about the need and essence of the operation and obtain consent for surgery.
Indications: 1) defect of the placenta or fetal membranes;
2) monitoring the integrity of the uterus after surgical interventions, long labor; 3) hypotonic and atonic bleeding;
4) childbirth in women with a uterine scar.
Workplace equipment: 1) iodine (1% iodonate solution);
2) cotton balls; 3) forceps; 4) 2 sterile diapers; 5) tray; 6) sterile gloves; 7) catheter; phantom; 9) consent form for medical intervention, 10) anesthesia machine, 11) propafol 20 mg, 12) sterile syringes.
3) forceps; 4) 2 sterile diapers; 5) tray; 6) sterile gloves; 7) catheter; phantom; 9) consent form for medical intervention, 10) anesthesia machine, 11) propafol 20 mg, 12) sterile syringes.
Preparatory stage of performing the manipulation.
1. Remove the foot end of Rakhmanov’s bed.
2. Perform bladder catheterization.
3. Place one sterile diaper under the woman in labor, the second on her stomach.
4. Treat the external genitalia, inner thighs, perineum and anal area with iodine (1% iodonate solution).
5. Operations are performed under intravenous anesthesia against the background of inhalation of nitrous oxide and oxygen in a 1: 1 ratio.
6. Put on an apron, sanitize your hands, put on a sterile mask, gown, and gloves.
The main stage of the manipulation.
7. The labia are spread with the left hand, and the right hand, folded in the shape of a cone, is inserted into the vagina and then into the uterine cavity.
8. The left hand is placed on the anterior abdominal wall and the wall of the uterus from the outside.
9. With the right hand located in the uterus, control the walls, placental area, and uterine angles. If lobules, fragments of the placenta, membranes are found, they are removed by hand
10. If defects in the walls of the uterus are detected, the hand is removed from the uterine cavity and transection, suturing of the rupture or removal of the uterus is performed (doctor).
Didn't find what you were looking for? Use the search:
Best sayings: If you get carried away with a girl, tails will grow; if you study, horns will grow.
9714 — | 7629 - or read all.
91.146.8.87 © studopedia.ru Not the author of the materials posted. But it provides free use. Is there a copyright violation? Write to us | Feedback.
Disable adBlock! and refresh the page (F5)
very necessary
In gynecology, different diagnostic methods are often used with and without instruments. The procedure is non-instrumental. Before starting, the woman in labor is given general anesthesia. An obstetrician-gynecologist performs a manual examination of the uterus after childbirth, inserting a hand into the reproductive organ for internal examination. The inspection method is considered quite informative.
Indications
The manipulation is carried out at the final stage of labor. During the procedure, the internal surface of the organ is examined and the condition of the walls is checked. When carrying out, compliance with all rules of asepsis is required. The doctor’s hands and the genitals of the woman in labor are carefully treated.
Preparation for the examination:
- the obstetrician removes urine with a catheter;
- the anesthesiologist administers anesthesia;
- The gynecologist treats the surface on the outside plus the inside of the thighs.
Manual examination of the uterus after childbirth is carried out if:
- there is bleeding;
- the placenta did not separate;
- labor took place naturally, whereas the previous one involved surgical intervention;
- 3rd degree cervical rupture;
- it is necessary to check the walls for integrity;
- loss of a baby during birth;
- the uterus has developmental defects;
- use of obstetric forceps.
The manipulation of the examination provokes a response from the reproductive organ. It begins to shrink more actively. When this does not happen, massage actions are carried out. The obstetrician massages the anterior wall with a clenched fist.
Manual examination of the uterine cavity after childbirth is accompanied by noticeable pain. Anesthesia is required. If epidural anesthesia was administered during labor, additional pain relief may not be given, in rare cases in a mild form.
Performing an inspection
During the examination, the doctor inserts a hand clenched into a fist into the vagina. Then it penetrates the uterine cavity to examine the internal state. The walls of the organ are felt and the density is studied. Particular attention is paid to the corners.
During manual examination, 3 types of anesthesia are used:
- inhalation;
- intravenous;
- extended regional.
During the examination, the position of the placental site is determined. If blood clots or membrane residues are detected, they are removed. If the placenta has not separated by this time, excretion occurs. Once the pieces have come out safely, manual exploration of the uterine cavity after delivery completes the process. Next, a gentle external-internal massage of the reproductive organ is performed.
- the general state of health of the woman in labor and the amount of blood loss are determined;
- anesthesia is administered;
- the obstetrician's hand enters the vagina, then inside the uterus;
- blood clots and remaining parts of the placenta, if any, are removed;
- the tone of the uterus and the integrity of the walls are determined;
- soft birth canals are examined;
- injuries are sutured if they occur;
- the condition of the woman in labor is re-evaluated;
- blood loss is compensated.
Sometimes it is not possible to remove the placenta using this method. A strong connection is diagnosed. Then the removal attempts stop. The woman in labor is moved to the operating room.
Peculiarities
The action is considered complex, traumatic, and large-scale. It takes a significant period of time. The unsatisfactory state of health of a woman in labor during the rehabilitation period is often associated with the consequences of anesthesia, and not with the intervention. Manual monitoring of the uterine cavity after childbirth performs 2 tasks:
diagnostic, therapeutic.
The first consists of analyzing the walls of the reproductive organ, establishing their integrity, and determining the remaining part of the placenta. The second is to stimulate the nerve endings of the muscular system using a gentle massage from the outside, from the inside.
To check the contractility of the reproductive organ, 1 ml of oxytocin is injected simultaneously with the beginning of the manipulation. If the test result is satisfactory, the massage actions continue.
After serious indications for examination, additional examination may be prescribed. The next step is to carry out therapy. The scheme is established individually for each woman in labor. The duration depends on the indications.
Treatment after the procedure:
- introduction of elements that increase uterine contractility;
- if large blood loss occurs, iron-containing drugs are prescribed;
- anti-inflammatory therapy is carried out;
- the immune system is strengthened;
- An ultrasound scan is performed during the postpartum period.
Source: https://vsedlyavasdamy.ru/info/ruchnoe-obsledovanie-matki-posle-rodov/
SURGICAL INTERVENTIONS IN THE FOLLOW-UP PERIOD
MANUAL SEPARATION OF THE PLACENTA
Manual separation of the placenta is an obstetric operation that involves separating the placenta from the walls of the uterus with a hand inserted into the uterine cavity, followed by removal of the placenta.
Manual removal of the placenta.
INDICATIONS
The normal afterbirth period is characterized by separation of the placenta from the walls of the uterus and expulsion of the placenta in the first 10–15 minutes after the birth of the child. If there are no signs of separation of the placenta within 30–40 minutes after the birth of the child (in case of partial tight, complete dense attachment or placenta accreta), as well as in case of strangulation of the separated placenta, an operation of manual separation of the placenta and release of the placenta is indicated.
METHODS OF PAIN RELIEF
Intravenous or inhalational general anesthesia.
OPERATIONAL TECHNIQUE
After appropriate treatment of the surgeon’s hands and the patient’s external genitalia, the right hand, dressed in a long surgical glove, is inserted into the uterine cavity, and the fundus is fixed from the outside with the left hand. The umbilical cord serves as a guide to help find the placenta. Having reached the place of attachment of the umbilical cord, the edge of the placenta is determined and, with sawtooth movements, it is separated from the wall of the uterus. Then, by pulling the umbilical cord with the left hand, the placenta is released; the right hand remains in the uterine cavity to conduct a control examination of its walls.
The delay of parts is determined by examining the released placenta and detecting a defect in the tissue, membranes, or the absence of an additional lobule. A placental tissue defect is identified by examining the maternal surface of the placenta, spread out on a flat surface. Retention of the accessory lobe is indicated by the identification of a torn vessel along the edge of the placenta or between the membranes. The integrity of the membranes is determined after they have been straightened, for which the placenta should be raised.
After the end of the operation, before removing the arm from the uterine cavity, 1 ml of a 0.2% solution of methylergometrine is injected intravenously at the same time, and then intravenous drip administration of drugs that have a uterotonic effect (5 IU of oxytocin) is started, an ice pack is placed on the suprapubic area of the abdomen.
COMPLICATIONS
In the case of placenta accreta, attempting to manually separate it is ineffective. The placental tissue ruptures and does not separate from the wall of the uterus, profuse bleeding occurs, quickly leading to the development of hemorrhagic shock as a result of uterine atony. In this regard, if placenta accreta is suspected, surgical removal of the uterus is indicated on an emergency basis. The final diagnosis is established after histological examination.
MANUAL EXAMINATION OF THE UTERUS
Manual examination of the uterus is an obstetric operation that involves examining the walls of the uterus with a hand inserted into its cavity.
Cleaning after childbirth: how does it happen, what are the reasons for scraping and the consequences of it?
Medical Consultant Surgery Cleaning the uterus after childbirth: everything you need to know about the procedure
The birth of a child is the happiest event for every woman.
It would seem that all the torment is behind us, this is happiness... Unfortunately, this is not always the case. After all, childbirth takes place in 2 stages: the birth of the baby and the birth of the placenta.
If the placenta is not born on its own, then the doctor has to remove it using other techniques, for example, curettage, vacuum aspiration.
- Modern methods of cleaning the uterus Curettage of the uterine cavity Manipulation techniques
- Further treatment tactics and possible complications
- Pain relief during curettage of the uterine cavity
- Vacuum aspiration Procedure technique
The main criteria for the success of uterine cleansing
The success of the curettage operation after childbirth is indicated (this is worth remembering!):
- absence of a significant increase in the body temperature of the postpartum woman (the norm is up to 37.5˚);
- no bleeding, moderate bleeding for several days (sometimes up to a week) is considered normal; it gradually turns brown and then becomes lighter; the discharge does not have an unpleasant odor;
- pain in the lower abdomen - it gradually decreases, but persists until the uterus contracts completely;
- the woman’s general condition is satisfactory, but slight dizziness may bother her; All these symptoms indicate that the cleansing is going well.
It is important to pay attention to the following symptoms and report them to your doctor:
- increased bleeding;
- complete absence of discharge in the first days after cleansing with a simultaneous increase in pain; this indicates a violation of purification;
- the discharge acquires an unpleasant putrid odor - a sign of infection;
- The temperature rises to 38˚ and above.
Complications of the 3rd period
30 minutes have not yet passed, but heavy bleeding has appeared from the uterus, indicating that the process of separation of the placenta has been disrupted. There is only one way out - manual separation of the placenta is necessary. It is performed by a doctor under inhalation or intravenous anesthesia by inserting his hand into the uterine cavity. There is no need to be afraid of this - if the child has already passed, then the doctor’s hand will even more so pass.
Manual separation of the placenta is also performed when 30 minutes have passed and there are no signs of placenta separation. But during these 30 minutes the doctor should not touch the uterus or put pressure on it in order to speed up the 3rd period. Just wait for signs of separation to appear, and then release the placenta by carefully tugging on the umbilical cord.
The placenta is subject to careful examination to determine the integrity of the placenta lobules and membranes.
If there is a defect in the placenta or is suspected, the doctor is required to perform a manual examination of the uterine cavity. Torn membranes are not an indication for this operation.
How is rehabilitation and recovery going?
For some time (4-6 days) after cleaning, the postpartum woman remains in the hospital under the supervision of a doctor. He conducts a daily examination to identify possible complications in a timely manner. Drug treatment is prescribed:
- medications to contract the uterus - this prevents recurrent bleeding;
- antibiotics - to prevent the development of infections.
If the rehabilitation period goes well, the woman is discharged 5-6 days after the cleansing, and further monitoring of her condition is carried out by a doctor at the antenatal clinic. Discharge after curettage (the same as after childbirth) continues for about 6 weeks, gradually becoming lighter and decreasing in volume. Two months after birth, complete cleansing and restoration occurs.
Early postpartum period
Yes, the birth is over, but we need to make sure there are no ruptures, that is, we have to examine the birth canal in the mirrors.
The cervix is carefully examined using special instruments, and ruptures are immediately sutured.
Tears in the soft tissue of the vagina are also sutured with self-absorbing threads; silk sutures are applied to skin tears, which are removed on the 5th day.
For 2 hours after birth, the postpartum woman remains in the delivery room under observation:
- Monitoring of well-being, pulse rate, blood pressure and the condition of the uterus is carried out.
- She wears an ice pack on her abdomen to maintain uterine hypothermia and prevent uterine bleeding.
This period is dangerous due to hypotonic bleeding, to stop which may require surgery to enter the abdominal cavity and possibly even remove the uterus.
Complications and consequences after uterine curettage
As with any other operation, complications are possible. Complications can be early or late. Early complications include:
- bleeding due to damage to a vessel located in the wall of the uterus; in this case, heavy bleeding may be from the genital tract, or may manifest itself in the form of hemometra - accumulation of blood in the uterine cavity due to the closure of the exit from the cavity; To prevent hemorrhage, antispasmodics are prescribed - medications that relieve spasms of smooth muscles;
- perforation (violation of the integrity) of the uterine wall with a sharp instrument - a small puncture can heal on its own, but a large one is sutured; As a rule, there are no unpleasant consequences.
These consequences are eliminated on the operating table or with repeated surgery within the first 24 hours. Modern clinics have every opportunity to cope with such consequences.
Late complications, which can develop after a few days after surgery and last a long time, include infection and associated consequences.
If the cleansing of the uterus is impaired, an infectious-inflammatory process develops - acute endometritis, which occurs with high fever, pain in the lower abdomen, and a change in the nature of lochia (they become foul-smelling, cleansing is disrupted).
Timely prescribed antibacterial therapy can quickly stop this process and prevent serious consequences.
Important! It is more difficult to cleanse and treat endometritis in women suffering from some hidden infections - chlamydia, ureaplasmosis, etc.
Therefore, obstetricians-gynecologists always insist on a full examination and treatment of infection during pregnancy planning. In such cases, endometritis becomes chronic and is accompanied by the development of adhesions.
The inflammatory process moves to the fallopian tubes and pelvic organs, where the consequences of inflammation - adhesions - also gradually develop.
Adhesions in the uterus and fallopian tubes are the main cause of infertility. Adhesions in the fallopian tubes can interfere with conception, and in the uterine cavity - with bearing a child and childbirth. The treatment of such processes is long-term. It begins with identifying and treating the infection, which, as a rule, with long-term inflammation, is mixed, caused by different pathogens.
After eliminating the infection, the adhesions are dissected, which is most often performed by endoscopic (without large incisions, using special endoscopic instruments) methods. And only after this the consequences of the infection are eliminated, and the woman can become pregnant again.
Source: https://MedLazaret.ru/ginekologiya/chistka-matki-posle-rodov.html
OPERATIVE INTERVENTIONS IN THE POSTPARTUM PERIOD
The postpartum period begins from the moment of birth of the placenta and lasts for 6–8 weeks. The postpartum period is divided into early (within 2 hours after birth) and late.
INDICATIONS
Indications for surgical intervention in the early postpartum period are: · rupture or incision of the perineum; · rupture of the vaginal walls; · cervical rupture; vulvar rupture; · formation of hematomas of the vulva and vagina; · inversion of the uterus.
In the late postpartum period, indications for surgical intervention are: · formation of fistulas; · formation of hematomas of the vulva and vagina.
CERVICAL RUPTURE
Based on the depth of cervical ruptures, three degrees of severity of this complication are distinguished. · I degree - tears no more than 2 cm long. · II degree - tears exceeding 2 cm in length, but not reaching the vaginal vault. · III degree - deep ruptures of the cervix, reaching the vaginal vaults or extending to it.
METHODS OF PAIN RELIEF
Restoring the integrity of the cervix in cases of I and II degree rupture is usually performed without anesthesia. For grade III rupture, anesthesia is indicated.
OPERATIONAL TECHNIQUE
The sewing technique does not present any great difficulties. They expose the vaginal part of the cervix with wide, long speculums and carefully grasp the anterior and posterior uterine lips with bullet forceps, after which they begin to restore the cervix. Separate catgut sutures are applied from the upper edge of the rupture towards the outer pharynx, with the first ligature (provisional) slightly above the rupture site. This allows the doctor to easily, without injuring the already damaged cervix, lower it when necessary. In some cases, a provisional ligature allows one to avoid the application of bullet forceps. To ensure that the edges of the torn neck are correctly adjacent to each other when suturing, the needle is injected directly at the edge, and the puncture is made at a distance of 0.5 cm from it. Moving to the opposite edge of the tear, the needle is injected at a distance of 0.5 cm from it, and the puncture is made directly at the edge. With this application, the sutures do not cut through, since the cervix serves as a gasket. After fusion, the suture line is a thin, even, almost invisible scar.
In case of a third degree cervical rupture, a control manual examination of the lower uterine segment is additionally performed to clarify its integrity.
VULVA RUPTURE
Damage to the vulva and vaginal vestibule during childbirth, especially in primigravidas, is often noted. With cracks and slight tears in this area, usually no symptoms are noted and there is no need for medical intervention.
OPERATIONAL TECHNIQUE
For ruptures in the clitoral area, a metal catheter is inserted into the urethra and left there for the entire duration of the operation. Then a deep puncture of the tissues is performed with a solution of novocaine or lidocaine, after which the integrity of the tissues is restored using a separate and nodal or continuous superficial (without underlying tissues) catgut suture.
RUPTURE OF THE VAGINAL WALL
The vagina can be damaged during childbirth in all parts (lower, middle and upper). The lower part of the vagina ruptures simultaneously with the perineum. Ruptures of the middle part of the vagina, as less fixed and more extensible, are rarely noted. Vaginal ruptures usually go longitudinally, less often - in the transverse direction, sometimes penetrating quite deeply into the peri-vaginal tissue; in rare cases, they also invade the intestinal wall.
OPERATIONAL TECHNIQUE
The operation consists of applying separate interrupted catgut sutures after exposing the wound using vaginal speculum. If there is no assistant for exposing and suturing vaginal tears, you can open it with two fingers (index and middle) of the left hand spread apart. As the wound in the depths of the vagina is sutured, the fingers that expand it are gradually pulled out. Suturing sometimes presents significant difficulties.
HEMATOMA OF THE VULVA AND VAGINA
Hematoma is a hemorrhage due to rupture of blood vessels in the tissue below and above the main pelvic floor muscle (levator ani muscle) and its fascia. More often, a hematoma occurs below the fascia and spreads to the vulva and buttocks, less often - above the fascia and spreads along the peri-vaginal tissue retroperitoneally (up to the perinephric region).
Symptoms of hematomas of significant size are pain and a feeling of pressure at the site of localization (tenesmus due to compression of the rectum), as well as general anemia (with an extensive hematoma). When examining postpartum women, a tumor-like formation of a blue-purple color is discovered, protruding outward towards the vulva or into the lumen of the vaginal opening. When palpating the hematoma, its fluctuation is noted.
If the hematoma spreads to the parametrial tissue, vaginal examination reveals the uterus pushed to the side and between it and the pelvic wall a fixed and painful tumor-like formation. In this situation, it is difficult to differentiate a hematoma from an incomplete uterine rupture in the lower segment.
Emergency surgical treatment is necessary for a rapid increase in size of the hematoma with signs of anemia, as well as for a hematoma with heavy external bleeding.
METHODS OF PAIN RELIEF
The operation is performed under anesthesia.
OPERATIONAL TECHNIQUE
The operation consists of the following stages: · tissue incision above the hematoma; · removal of blood clots; · ligation of bleeding vessels or suturing with 8-shaped catgut sutures; · closure and drainage of the hematoma cavity.
Who needs an ultrasound after childbirth and when, how it is done and interpreted
› Ultrasound during pregnancy
07.05.2019
During the postpartum period, a woman’s body needs to quickly rebuild, adapt to blood loss, restore the size of the uterus, and begin lactation. An ultrasound after childbirth helps doctors track how the mother’s body is coping with the restructuring, whether there are any malfunctions, or whether help is needed.
Indications and contraindications
All women in labor undergo an ultrasound on the 3rd day after birth - before discharge, doctors check that the uterus is contracting, there is no risk of bleeding, and the suture is intact. If necessary, an ultrasound is performed on the 1st day.
There are no contraindications, because ultrasound is a safe and informative way to monitor the condition of the genital organs in the postpartum period.
Indications for emergency postpartum ultrasound examination are:
- bleeding in the early postpartum period;
- soreness and redness of the postoperative suture, purulent discharge;
- manual examination of the cavity after childbirth;
- the appearance of excessively abundant, unpleasant-smelling vaginal discharge;
- temperature rise above 38 °C (measure at the elbow);
- severe pain in the lower abdomen in the first days after childbirth.
After a caesarean section, if there is no cause for concern, the examination is also carried out on the 3rd day. They evaluate not only the condition of the genital organs, but also the condition of the suture. After a caesarean section, the uterus contracts more slowly, but if the process continues, no intervention is required. You can become pregnant again after the suture has completely healed and is completely intact, usually after 1.5–2 years.
1 month after giving birth, you must go to the antenatal clinic; if necessary, the doctor will refer you for a repeat examination. If there are no complaints or fever, the discharge has stopped, then the appointment proceeds as usual. It is usually recommended to start taking birth control.
Watch a video review from a gynecologist on this topic:
How to prepare for research
Before the examination, you are usually warned that the bladder must be full. In rare cases, when ultrasound is necessary for emergency reasons, fluid is injected into the bladder through a catheter.
Bring a towel and diaper with you. A towel will be needed to wipe the gel after the examination, and a diaper will be placed on the couch.
How an ultrasound is performed on women after childbirth
The study is carried out through the abdomen, using a transabdominal sensor. A special gel is applied to the skin so that the ultrasound is not distorted. The sensor is moved along the abdomen, examining the uterus, appendages (fallopian tubes and ovaries), postoperative suture, and the condition of the abdominal cavity.
During the examination in the maternity hospital, they look at the size of the uterus, whether there are any pathological contents, and how it contracts. The procedure takes on average 10 minutes.
Before discharge from the maternity hospital, they always look at not only the results of the study, but also the tests, the condition of the sutures, and body temperature. If everything is in order, the woman is sent home.
Interpretation of postpartum ultrasound results
Criteria for the normal state of the uterus according to ultrasound in the postpartum period (3rd day):
- The shape is close to spherical, the tone is increased.
- The cavity is slit-like, with clear contours, width in the upper part is up to 1 cm, in the lower part up to 1.5 cm.
- A small number of blood clots are acceptable.
- The bottom above the pubic symphysis is at a height of 10–13 cm.
- The endometrium (inner layer of the uterus) has a folded structure.
- Weight about 600–700 g.
- At the site of placental rejection there is a rough wound surface with thrombosed vessels.
- A small amount of gas and decidual tissue (the layer between the placenta and uterus) is torn away is acceptable.
- The normal size of the uterus is: length 125–135 mm, width 120–130 mm, anteroposterior size 65–68 mm.
Pathology by ultrasound:
- Subinvolution of the uterus is a pathological slowing of contractions. On ultrasound, the size exceeds the norm, there are hyperechoic (dark gray) inclusions in the cavities (a large number of blood clots and placental remnants). This condition can lead to infection. The shape of the uterus is spherical.
- Signs of endometritis (infection of the uterine cavity) - ultrasound reveals a decrease in tone (thinning of the uterine wall), a large number of blood clots, placental tissue, accumulation of gases in the cavity (looks like a hypoechoic formation - light gray, white).
- Remains of placental tissue and membranes can cause postpartum hemorrhage; it is important to remove them in time. Bleeding may also occur 6–8 weeks after birth.
Also see ultrasound pathology after childbirth:
How much does a postpartum ultrasound cost?
Ultrasound after childbirth is free and is performed in the maternity hospital for all postpartum women. If you wish, you can undergo examination for a fee in a private clinic. Prices vary from 600 to 2000 rubles.
Never refuse to undergo testing after delivery; complications from infection and bleeding can be fatal. Mom's health is very important, especially for a newborn baby.
Share the article, leave comments with your experience. Did you have an ultrasound after childbirth and when? All the best.
Who needs an ultrasound after childbirth and when, how it is done and interpreted Link to main publication
Source: https://uziman.ru/pri-beremennosti/uzi-posle-rodov
Manual examination of the uterine cavity, technique, complications
The uterus is an unpaired organ consisting of smooth muscles, responsible for the gestation and development of the embryo. Location of the uterus: small pelvis. Next to the uterus is the bladder and rectum. Downwards the uterus is rounded, passing into the cervix. This is a mobile organ. Moreover, its position directly depends on the position of the bladder and rectum.
Manual examination of the uterine cavity is impossible if the bladder is full. Also, in preparation for examination by a specialist, it is necessary to empty the rectum. The presence of feces in it will not allow a specialist to conduct a full examination.
What is a manual examination of the uterine cavity?
Examination without the use of any foreign objects or technologies - manual examination. This is an operation that requires maximum hygiene. That is, before starting such a procedure, the doctor must thoroughly treat the hands and uterine cavity with an antiseptic.
A specialist conducts such an examination if there are certain indications. Manual examination of the uterine cavity after childbirth is also indicated.
Indications for manual examination of the uterus
During the postpartum period, manual examination is mandatory. Doctors pay special attention to women in labor whose placenta does not leave the organ cavity within 30 minutes. This phenomenon is considered an indication for manual separation of the placenta.
Experts also identify the following indications for conducting a manual examination:
- bleeding in the uterine cavity;
- postoperative period;
- retained placenta inside the uterus after childbirth;
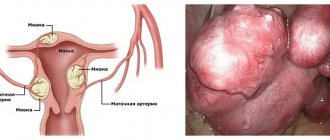
- fibroids;
- scarring of the organ;
- defects in the development of the amniotic membrane.
Experienced specialists know that manual examination of the uterine cavity must be of high quality. To do this, you need to move your hand in a circle, feeling the surface of the organ. Otherwise, there is a possibility that only one side will be thoroughly examined - the one that was under the doctor’s palm.
After a complete manual examination, women who have just given birth are often prescribed additional curettage.
This procedure is necessary in order to completely cleanse the uterus of the remnants of the placenta.
Indications for manual examination of the uterus may be more serious, but in such cases additional examination and then treatment are prescribed. You cannot self-medicate in such cases.
It is necessary to seek help from qualified specialists and strictly follow their recommendations.
Technique for manual examination of the uterine cavity
Before examining the patient, the doctor must treat his hands with an antiseptic. Also treat the surface of the organ being examined - the uterus. Then the doctor puts a sterile glove on his right hand and inserts it into the organ cavity.
At the same time, he holds its bottom with his left hand. If a doctor is examining a patient who has just given birth, he must check the uterus for the presence of placental remains and remove them if necessary. Depending on the patient’s condition, the doctor decides on pain relief before the procedure.
If an anesthetic was administered before delivery, the patient does not need additional anesthesia. Upon completion of the examination, it is necessary to administer oxytocin to improve uterine contractility. This must be done until the doctor removes his hand from the organ being examined.
Complications
One of the main and most serious consequences during manual examination of the uterine cavity may be the accretion of the placenta to the walls of the organ. Then a specialist, when trying to separate it manually, must be prepared for the possibility of bleeding, which often leads to dire consequences due to the negligence of doctors.
To avoid this, an experienced doctor recommends surgery to remove the uterus. Such an operation is not a death sentence today. And there are many ways to preserve the reproductive organ. However, you need to carefully monitor women's health and regularly undergo examinations by a gynecologist and other specialists.
Prevention
Preventive measures will also help to avoid many troubles related to women's health. For example, periodically you need to take vitamin complexes that are aimed at preserving women’s health. Also today, special exercises that help strengthen the uterus and its cervix are very popular.
Source: https://FB.ru/article/392444/ruchnoe-obsledovanie-polosti-matki-tehnika-oslojneniya
Prevention
Preventive measures will also help to avoid many troubles related to women's health. For example, periodically you need to take vitamin complexes that are aimed at preserving women’s health. Also today, special exercises that help strengthen the uterus and its cervix are very popular.
In gynecology, different diagnostic methods are often used with and without instruments. The procedure is non-instrumental. Before starting, the woman in labor is given general anesthesia. An obstetrician-gynecologist performs a manual examination of the uterus after childbirth, inserting a hand into the reproductive organ for internal examination. The inspection method is considered quite informative.
Manual examination of the uterus after childbirth
The uterus is an unpaired organ consisting of smooth muscles, responsible for the gestation and development of the embryo. Location of the uterus: small pelvis. Next to the uterus is the bladder and rectum. Downwards the uterus is rounded, passing into the cervix. This is a mobile organ. Moreover, its position directly depends on the position of the bladder and rectum.
Manual examination of the uterine cavity is impossible if the bladder is full. Also, in preparation for examination by a specialist, it is necessary to empty the rectum. The presence of feces in it will not allow a specialist to conduct a full examination.