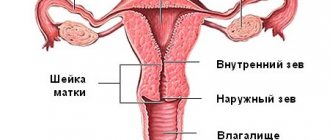
The uterus is the main organ that distinguishes a woman from a man. It is thanks to their physiological characteristics that representatives of the fair sex can bear and give birth to a healthy baby. The uterus is a hollow muscular organ that is divided into three parts: the cervix, the body and the fundus. By looking at the cervix, the doctor can determine whether labor will begin soon.
Cervix during pregnancy
The cervix connects the vagina and uterus. Outwardly, it resembles a tube. If the pregnancy is progressing normally, the cervix will have a firm consistency, preventing the fertilized egg from descending too low. The cervical canal should be tightly closed. The cervix in the early stages does not indicate the beginning of pregnancy. If suspicious discharge appears, the expectant mother should immediately consult a doctor.
The cervix begins to change its structure and shape only a few weeks before birth. It is thanks to such changes that the child will be able to move almost unhindered through the birth canal. Dilatation of the cervix long before the expected date of birth is a bad sign. At best, premature birth will begin, at worst, the woman will lose the child.
If the cervix opens prematurely
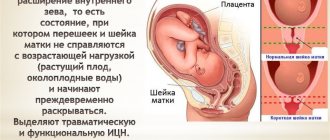
The opposite situation also happens, when the cervix begins to open and prepare for childbirth ahead of schedule. This is usually associated with a pathology of the cervical canal called isthmic-cervical insufficiency. It lies in the inability of the cervix to properly contain the fetus. It shortens and opens early, which often leads to spontaneous abortion.
The presence of this pathology is indicated by the length of the cervical canal at 20–30 weeks of less than 25 mm.
Isthmic-cervical insufficiency can develop due to trauma to the cervix, hormonal disorders, or excessive load on the cervix during pregnancy.
In this situation, measures should be taken aimed at maximizing the prolongation of pregnancy:
- Bed rest (usually in a hospital setting).
- Prescription of tocolytics, antispasmodics and sedatives.
- Emotional peace.
- Stitches are placed on the cervix, which are removed at 37 weeks.
In addition, treatment is carried out to promote the rapid maturation of the fetal lungs in case labor begins prematurely. Before childbirth, the cervix changes so much that it allows the baby to be born unhindered.
The gradual dilatation of the cervix before childbirth is almost unnoticed by the woman herself.
Therefore, visits to the gynecologist in the third trimester should be regular and accompanied by a vaginal examination, which allows you to assess the degree of readiness of the body for childbirth. This is especially true for those women who already feel other warning signs. If the due date has already approached, but cervical maturity has not yet arrived, then there is no need to be afraid of stimulation. Sometimes delay can cost the lives of both mother and child.
Also read: Can there be a discharge in early pregnancy?
I was on DO for 2 weeks. As soon as I arrived, they immediately rushed me to the chair and let me “examine” my cervix with the words: “Be patient, the more often and more thoroughly we examine you, the easier it will be for you to give birth.” To say that it was painful is to say nothing. Especially when the doctor said that the cervix was “fucked up”, so hard, it could barely let one finger through.” Before giving birth, she never softened, and as a result - ECS.
I was on DO for 2 weeks. As soon as I arrived, they immediately rushed me to the chair and let me “examine” my cervix with the words: “Be patient, the more often and more thoroughly we examine you, the easier it will be for you to give birth.” To say that it was painful is to say nothing. Especially when the doctor said that the cervix was “fucked up”, so hard, it could barely let one finger through.” Before giving birth, she never softened, and as a result - ECS.
Some kind of sadism :( During my first pregnancy, I was in prenatal care, they looked at me often, sometimes it hurt a little, but nothing more. As usual, everything depends on the doctor. It’s like with injections: someone injects you and you won’t notice, but another - your whole butt will hurt :(
So I agree. Only here (in the UK) they don’t look, they don’t go there at all during pregnancy.
At the last appointment, in response to my request to look at readiness, the midwife widened her eyes and said that this would only happen in the maternity hospital, when you arrive for the birth. And they only take people for childbirth when the process is already in full swing. I'm sitting here in anticipation and uncertainty. 027:
So, in general, pregnant women are not examined unnecessarily - feeling your cervix can trigger the onset of labor, so they examine the cervix either when there is a suspicion of the onset of labor, or you are already 41+ weeks and you are still not giving birth and not giving birth. Usually such manipulations are carried out already in the RD. They cannot help but look because otherwise they cannot determine whether there is an opening or not.
I agree that everything seems to depend on the doctor
they looked at me, it was certainly not pleasant :073: but it was quite tolerable, there was no severe pain, in a minute you won’t even remember
It all depends on the doctor. It seems to me that there are doctors who specifically try to make it more painful. And if the doctor is a normal person, there is practically no pain, just unpleasant sensations.
horror. I'm scared already. Especially after my friend said that in the whole process of childbirth, the most painful thing for her was the examination of the cervix.
While I was in prenatal care (5 days), I was examined every day. Absolutely no unpleasant sensations. During the birth process, too, repeatedly, also calmly. But I was always examined by the doctor who gave birth to me. And once or twice it was unpleasant.
It all depends on the doctor. It seems to me that there are doctors who specifically try to make it more painful. And if the doctor is a normal person, there is practically no pain, just unpleasant sensations.
sometimes during the examination, especially if during childbirth and poor dilation, the doctor probes her more “intensely” to speed up the process of dilatation - this can cause painful sensations - here, who has what approach and who was taught how.
At my institute, obstetrics was taught in different places and with different teachers - so everyone preaches their own. Some people say it’s better to actively “watch” than to once again stimulate it with medication. someone is the opposite and you are. so it’s not even a matter of the doctor’s sadistic inclinations often.
brrr. yes, just in a week for a cervical examination :(
So I agree. Only here (in the UK) they don’t look, they don’t go there at all during pregnancy.
At the last appointment, in response to my request to look at readiness, the midwife widened her eyes and said that this would only happen in the maternity hospital, when you arrive for the birth. And they only take people for childbirth when the process is already in full swing. I'm sitting here in anticipation and uncertainty. 027:
But if they looked at you and said “one finger is open,” what would be more definite then? Some girls with such dilatation survive for several weeks.
I'm actually interested too. I vaguely remember that somewhere someone mentioned that at some course, at Rainbow, or maybe not, they were taught this.
Let the doctor take a look. I'm more scared if he doesn't look.
One of my friends. without looking, they injected Ott with a sleeping pill, and five minutes later they looked - it’s time for you to push. As a result, she fell asleep while pushing, and this affected the baby.
More to read: Ktg how many movements should there be
If I could look, I could scream - I already have 9 fingers open, I don’t need your sleeping pills.
if it didn’t occur to her at that moment, BEFORE the sleeping pills, to ask the doctor about dilatation, then. I don’t think it would come to hunch over, reach inside yourself with your hand and feel the opening. 008:
and they ask “is there anyone in the house” :046:
horror. I'm scared already. Especially after my friend said that in the whole process of childbirth, the most painful thing for her was the examination of the cervix.
Maybe they opened her neck with their hands? I know that in some cases doctors do this. They did it to a friend - she says the pain is hellish.
During my labor, the most painful thing was the dilation examination, because they look at the peak of contraction. I suspect that the doctor opened it a little with her hands, she just didn’t comment, it was as if she was turning it with her hand. horror, horror, how painful it was.
And just when examined on the chair before childbirth, it is not very painful, but sensitive and unpleasant.
Why does the cervix change its structure ahead of schedule?
Pathological changes in the uterus occur for a number of reasons. The risk group includes women who have once had an abortion or miscarriage. Cervical erosion, as well as injuries associated with previous births, can also cause the pharynx to open long before the desired date. In addition, hormonal disorders, such as progesterone deficiency, lead to changes.
The expectant mother herself may notice changes in the early stages of pregnancy. Mucous discharge of a yellowish tint indicates that the cervix is open. Whether this is normal or not, only a doctor can tell you. Therefore, a pregnant woman should immediately report any suspicions to a specialist.
How is stripping done?
The membranes of the amniotic sac are separated manually when the cervix is at least slightly dilated, usually combining this with examination and assessment of the condition of the cervix and vagina.
The doctor inserts a finger into the opening of the cervix and rotates it in a circle, separating the membranes of the amniotic sac (amniotic membrane) from the walls of the uterus and mechanically expanding it, forcing the cervix to open. Those who have gone through forced cervical dilatation and membrane stripping usually do not forget about this. The procedure is painful, although not comparable to the pain of childbirth. However, if you can find out about the sensations during childbirth in advance and tune in to the pain, then usually no one reports the pain of stripping. Moreover, in most cases, the doctor or midwife gives no warning at all about what they are going to do and leaves the patient no choice. Sometimes you can find out in advance about the upcoming procedure, for example, by the words “Now relax, I’ll take a good look at you” or promises that after the examination the plug may come off and the onset of labor will speed up. But the fact that a medical procedure is to be performed, it has a name, indications, contraindications, and can cause complications, is usually not reported. But the patient not only has the right to know why stripping is dangerous, but also to agree or refuse it.
Cervical dilatation
The longer the pregnancy, the more the connective tissue of the cervix is replaced. Young fibers are more elastic. Thanks to this, the cervix opens quite strongly before childbirth, allowing the fetus to come out. The organ shortens and becomes looser.
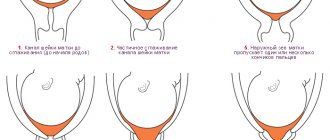
Softening of the cervix before childbirth occurs gradually. This process begins from the 32nd week of pregnancy. For first-time mothers, preparation takes a little longer. Dilation begins from the internal os of the cervix. Gradually, the fetus moves outward, stretching the external pharynx. In women who give birth repeatedly, the cervix dilates much faster. For some pregnant women, this process may take only a few hours. By the end of pregnancy, the external cervical os may already be open to several fingers.
What problems might arise?
From the 37th week of pregnancy, the uterus is completely ready for childbirth. But this alone is not enough. Many women are so afraid of giving birth that they psychologically slow down the process. Fears prevent the production of hormones necessary for softening. The cervix remains firm before birth. If stimulating actions do not lead to the desired changes, the doctor may prescribe a cesarean section.
Regular labor is required for normal cervical dilatation. If the contractions are too weak, the uterus may remain at the prenatal level. Quite often, such a nuisance occurs with polyhydramnios or insufficient amniotic fluid. When the uterus is overstretched, its tone, that is, contractility, decreases. As a result, labor also weakens, and the cervix opens less intensively.
The risk group includes women who give birth for the first time after 35 years. The main reason for poor opening may be a decrease in tissue elasticity. Your doctor will examine your cervix before giving birth. If the organ does not have the structure necessary for this time, surgical intervention will be required.
Procedures to prepare for the day of birth
If a woman enters the maternity hospital with contractions or broken waters, the algorithm of actions and all procedures before childbirth are described in the previous paragraph.
But a pregnant woman may be in the pregnancy pathology department and her delivery may be planned, or contractions may begin at any time. In this case, she expects the following:
- Examination by the attending or duty doctor, and, if necessary, by the head of the department.
- CTG recording - fetal heartbeat.
- Cleansing enema and shower.
- Transfer to an observational or physiological maternity ward.
If a woman is planning a caesarean section, the procedure is the same. A light dinner is allowed the night before; in the morning you can only drink a little clean water.
Also, the pregnant woman must collect all her things if she was previously in the pathology department. Some can be taken with you to the delivery room, the other will need to be put in a storage room.
Watch this video about preparatory procedures before childbirth:
In the delivery room
The maternity room includes an examination room (usually several), prenatal wards where women are during contractions, as well as the maternity rooms (halls) themselves - they contain special chairs, a table for treating a newborn, as well as equipment and tools that may be needed during childbirth, everything is sterile, and consumables are disposable (diapers, etc.).
The delivery room also includes an operating room, where, if necessary, a woman can be sent urgently during childbirth.
After admission to the delivery room, the woman is assigned to one of the prenatal wards, where she will be monitored (including video), and CTG monitoring of the fetal condition is carried out. The doctor, who is in charge of the delivery room at this time, clarifies the woman’s complaints and medical history, studies the birth chart and, if necessary, conducts an examination in a gynecological chair.
If childbirth proceeds without complications, then the frequency of vaginal examinations is as follows:
- every four hours during labor;
- after the rupture of amniotic fluid;
- if complications are suspected.
The woman is in the prenatal ward throughout the contractions; she is also allowed to move along the corridor and take a shower (as a method of pain relief).
With the beginning of the pushing period, the issue of transfer to the delivery room itself is decided. Here the woman lies down on a chair, the doctor monitors the condition of the fetus by heart rate (listened to with a stethoscope or CTG monitor).
After the birth of the child, the birth canal is examined for rupture. If necessary, the doctor performs suturing, as well as additional manipulations. For another two hours, the woman is under close supervision of medical personnel for timely detection of complications. After which the postpartum woman is transferred to a ward with the baby.
If an emergency or planned caesarean section is performed, then immediately after the operation the woman is transferred to the intensive care unit for observation - for at least two hours, most often for 12-24 hours. After this, she is also transferred to the postpartum ward.
Watch this video on how to care for a suture after a caesarean section:
Preparing the cervix for future births
Shortly before the expected date, the doctor will examine the woman in labor. If the cervix is immature, it is necessary to carry out stimulating actions that will help release the necessary hormones and prepare the body for childbirth.
All such methods can be divided into medicinal and non-medicinal. With the help of medications prescribed by a doctor, it is possible to prepare the uterus for childbirth only in a hospital setting. All actions must be performed under the strict supervision of a physician. The introduction of kelp sticks into the cervical canal is considered effective. This is done immediately before the expected date of birth. Under the influence of heat and moisture, kelp swells, affecting the organ. In addition, seaweed secretes substances that promote cervical ripening. In the best case, labor can begin within 5-6 hours.
Synthetic prostaglandin, which is introduced into the vagina in the form of a gel or suppository, can also stimulate the opening of the cervix. The desired effect can be achieved within a few hours.
How is the birth process going?
After the water breaks and the head is inserted, to assess the correspondence of the size of the fetal head to the mother’s pelvis during labor, the doctor must check Vasten’s sign and can inform the expectant mother about the results. The woman lies on her back. The doctor places one palm on the surface of the symphysis pubis, the other on the area of the presenting head. If the sizes of the mother's pelvis and the fetal head correspond, the anterior surface of the head is located below the plane of the symphysis (pubic symphysis), i.e., the head extends under the pubic bone (Vasten's sign is negative). If the anterior surface of the head is flush with the symphysis (flush Vasten's sign), there is a slight size discrepancy. If there is a discrepancy between the sizes of the mother's pelvis and the fetal head, the anterior surface of the head is located above the plane of the symphysis (Vasten's sign is positive). A negative Vasten sign indicates a good match between the sizes of the woman’s head and pelvis. With the second option, a favorable outcome of childbirth through the natural birth canal is possible, subject to certain conditions:
- good labor activity;
- average fruit size;
- no signs of post-maturity;
- good fetal condition during childbirth;
- presence of light waters;
- good configuration of the head and its correct insertion when passing through the pelvic cavity.
A positive sign indicates that the mother’s pelvis is an obstacle to the passage of the fetus and natural childbirth is impossible in this case.
During a vaginal examination, the doctor evaluates how the fetal head is positioned. If everything goes well, then most likely you will not hear anything from the doctor on this score; if he wants to emphasize that everything is normal, he will say that the fetus is occipital presented. Normally, the fetal head descends into the pelvic cavity in a state of flexion, that is, the baby’s chin is pressed to the sternum, and the point in front of the birth canal is the back of the fetal head. In this case, it passes through all the planes of the pelvis with its smallest circumference quite easily. There are incorrect types of cephalic presentation, when the head is extended and either the forehead or the face of the fetus enters the pelvic cavity first. These types of cephalic presentation are called frontal and facial. In these cases, childbirth often ends with a cesarean section in order to reduce trauma to the fetus and mother. But with a small degree of extension of the head, good labor activity, and small size of the fetus, natural delivery is possible.
A woman may hear the expressions “front view”, “rear view”. No worries. With a cephalic presentation, this means that in the anterior view, the back of the fetal head faces the anterior wall of the uterus, and in the posterior view, it faces backward. Both options are normal, but in the latter case the pushing lasts longer.
After an external vaginal examination, the doctor can tell you how the head is moving through the birth canal.
The head is pressed against the entrance to the pelvis. Two weeks before the onset of labor in primiparous women, the fetal head begins to descend and press against the entrance to the pelvis. Due to this, pressure on the lower segment and cervix increases, which promotes the ripening of the latter. In multiparous women, the head drops 1-3 days or even several hours before the onset of labor.
The head is a small segment at the entrance to the small pelvis. In this obstetric situation, the head is motionless, its largest part is located above the plane of the entrance to the pelvis, it can still be palpated through the anterior abdominal wall. This happens in the first stage of labor - during contractions.
The head is a large segment at the entrance to the small pelvis. In this case, it is located with its large circumference in the plane of the entrance to the small pelvis; it can hardly be felt through the anterior abdominal wall, but during a vaginal examination the doctor can clearly identify it, as well as all the sutures and fontanelles. This is how the head is positioned at the end of the first stage of labor before pushing begins.
The head in the pelvic cavity is not detected during external examination; during vaginal examination, the doctor sees that it fills the entire pelvic cavity. This obstetric situation is observed during the pushing period.
Puncture of the amniotic sac
There are radical methods to stimulate labor. First of all, these include piercing the amniotic sac. If the cervix does not dilate properly during labor, your doctor may perform an amniotomy, which will cause your water to break. Thanks to this procedure, the fetal head descends and begins to put pressure on the cervix. If additional medications are used, labor will begin to proceed much more intensely.
A cleansing enema also has excellent stimulating properties. It is no coincidence that this procedure is mandatory when a woman is admitted late into the maternity ward. The enema irritates the back wall of the uterus, stimulating contractions. Quite often after this, the mucous plug comes out. In this case, the cervix opens much faster before childbirth. It is worth noting that an enema is only appropriate for those women who have already reached their expected date. Stimulation before this period can be dangerous for the baby.
What are the dangers of examining “with passion”?
When separated, the lower part of the amniotic membranes is “peeled off” from the cervix and walls of the uterus. Both the insertion of the finger and the manipulation cause painful sensations, then the lower abdomen may “ache,” blood may be released, and the mucous plug, which protects the cervix and the uterus itself from infection, may come off. Normally, this is considered a harbinger of labor, but with stripping it is a consequence of manipulation. What else could it be?
- Cervical injury if dilatation is assessed incorrectly or the doctor performs the procedure incorrectly.
- Bleeding due to early and too rapid detachment of membranes, expansion of the cervical canal.
- The introduction of infection from the vagina or its subsequent independent penetration, since the plug comes away and there is nothing left to protect the amniotic sac and the child from bacteria.
- The outpouring of water may begin without the birth itself, which is dangerous due to the anhydrous period, and subsequent stimulation during labor, and infection of the fetus.
- Moreover, if desired, you can deliberately open the bladder or administer a drug to locally stimulate the onset of labor, and do this unnoticed by the woman.
Stripping is not noted in the medical record. Inspection - yes, but the actual manipulation of the membranes and neck - no. This is an unofficial, although popular, method of inducing labor, and it will not be noted in the documents. This means that in case of complications, it will be impossible to find the culprit.
Despite the impressive list of disadvantages and possible complications, stripping is considered the gentlest and most natural method for stimulating the birth process. For example, if the pregnancy has been delayed and the cervix is already open, or labor has begun, but is going slowly, and you need to speed it up a little. Therefore, it is worth resorting to in a situation where stimulation is definitely needed. But this must be done consciously.
Non-drug stimulation
If the pregnancy is already more than 40 weeks, and labor does not occur, some methods will help to stimulate it at home. The natural way can be called sexual intercourse. Sex promotes contraction of the walls of the organ, due to which the cervix opens much faster before childbirth. In addition, semen contains hormones that promote the onset of labor. Sexual intercourse is undesirable only if the mucus plug has already come off. The risk of infection increases.
Physical activity also contributes to the speedy onset of the process. Simple activities lead to more intense dilatation of the cervix before childbirth (a photo of a happy mother can be seen in the article). Physical activity should be fairly moderate. If possible, a pregnant woman should sign up for special gymnastics long before giving birth.
Long walks, climbing stairs, and cleaning the house stimulate the onset of labor just as well as special exercises.
Inspection algorithm
A week before the due date of the baby, you need to visit a gynecologist to find out about the condition of the uterus. When examining pregnant women in a chair before childbirth, they first study the external organs, and then the condition of the internal ones, paying attention to the labia.
Is it painful to look at the cervix before childbirth? It depends on the condition of the organ and whether there are gynecological problems. During a normal pregnancy, a woman feels discomfort. Complications during pregnancy lead to pain and discharge.
How to examine the cervix before childbirth:
- take a comfortable position in a chair;
- examine the genitals;
- determine the condition of the skin;
- mirror study;
- uterine size;
- the nature of the discharge;
- smear on flora.
The inspection is carried out in two stages: using mirrors and manual examination. After assessing the skin and mucous membranes, they move on to the perineum and urethra. Speculums will hold the vagina open to reveal the presence of infections and the condition of the cervix. Then they move on to manual inspection. The gynecologist inserts the middle and index fingers of one hand. And he puts the other one on his stomach. The shape of the uterus, location, correspondence to the timing of pregnancy, the surface of the sacrum and the walls of the pelvis are examined.
Can a chair examination trigger labor? No. They will begin if the time has come. The process will help determine the condition of the fetus and the readiness of the woman’s body for childbirth. When the uterus begins to open and the gynecologist conducts an examination, the plug comes out and brown discharge appears. Labor may begin in 2–3 days.
Some women have a very painful prenatal exam because they don't relax. The gynecologist uses folding speculums in the vagina, examines the cervix, and then the walls of the organ when removing the instrument. Performs the procedure using spoon-shaped mirrors. To do this, insert the lower part for the back wall, and then the upper part to view the front.
Family support is an important element of a successful birth
The psychological attitude of the expectant mother is of great importance. Problems and fears about childbirth can lead to serious problems. It is within the power of loved ones to help a pregnant woman tune in to a successful outcome of events. In the last month, it is advisable to protect the expectant mother from family problems. Let her think only about the next meeting with the baby.
Childbirth is much easier for women with a husband or other loved one nearby. The right attitude and doctor’s recommendations will help to give birth to a healthy and strong baby.