Every woman planning to become a mother experiences excitement - after all, this is one of the most important periods in her life. It would seem that this is a natural process that has been around for several thousand years, but expectant mothers still often have questions and fears about the upcoming birth.
In some cases, a pregnant woman may hear from a doctor about the dangers of premature cervical dilatation. To allay fears about this and find out? How to maintain the health of mother and baby in this situation, let's figure out what this means.
Features of the structure of the uterus
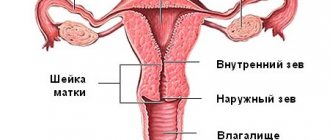
The uterus is a smooth muscle hollow organ, shaped like a pear, and includes the following components: the body of the uterus, its cervix and the fundus of the uterus. Mainly, the uterus is designed to bear a child. If you imagine it in the shape of a pear, then its narrower part - the cervix - will be located at the bottom, and the fundus of the uterus, on the contrary, will be at the top. The cervix is part of the uterus itself and is a muscular tube that originates from the uterus and opens into the vagina.
The uterus itself is located in the pelvic cavity between the bladder and rectum. The developing fetus puts pressure on the walls of the bladder, which is why pregnant women experience frequent urges to go to the toilet. In a normal state, the uterus is tilted forward, and is surrounded on both sides by special ligaments that help support it, preventing it from descending, on the one hand, and on the other, providing it with a minimum of movement. These ligaments help the uterus respond to changes in neighboring organs: tilt back or forward when the bladder or rectum fills, and rise up during pregnancy.
The cervix completes the uterus and connects it to the vagina. The cervix reaches approximately one third of the entire length of the uterus. The shape of the cervix differs between nulliparous women and women who have children. In women who have given birth, the cervix is round or resembles a truncated cone. In nulliparous women, it is flatter and cylindrical in shape. In addition, the shape of the cervix changes after an abortion.
Signs of approaching labor
The next sign is the release of water that surrounds the baby in the stomach. They can pour out either in a stream or gradually. Along with this, the mucous plug comes out, which during pregnancy blocks the main exit channels. It is impossible to independently determine its conclusion, because the plug often takes the form of amniotic fluid. As soon as the cervix begins to change, then the plug will come out.
The duration of labor begins from the moment the cervix begins to dilate and ends with the birth of the child. Typically, dilatation occurs during intense contractions. Since each organism has its own characteristics, the timing of contractions is different. The stronger and more intense the contractions, the faster the cervix will open.
The weight of the fetus and its activity also play an important role. In addition, you need to pay attention to the mother’s hip system, the elasticity and physical condition of the mother’s uterine muscles. The total duration for a primigravida woman is from 15 to 24 hours, in other cases - up to 12 hours. It is also worth taking into account the age of the woman in labor, since the younger the woman, the faster and more intensely the cervix contracts. To make childbirth easier and less time-consuming, it is necessary to attend special courses during pregnancy that teach proper breathing and relaxation.
You can learn more about the approaching birth by watching this video:
Muscle contraction
In order for a child to see our world, the cervix must be fully dilated, and for this it must be smoothed out. By smoothing we mean shortening, that is, expanding the internal pharynx. During contraction, pressure is applied to the neck, due to which the muscles tense and the muscle fibers become compacted, namely the walls thicken.
Contractions begin in the uterine day, so these are the thickest places. Since these compactions occur both in the uterine fundus and in the upper segment, the muscles pull the cervix up and to the side, so the lower element of the uterus becomes thinner and smoother and the cervix is fully dilated.
All these actions increase intrauterine pressure, which, in turn, puts pressure on the amniotic sac. As a result of this, amniotic fluid is directed to the internal os of the uterus, precisely to the place where there is no resistance. Due to excessive pressure, the lower pole of the fetus separates from the uterus and rushes into the cervix of the internal os. Thus, the amniotic sac tightens and the cervix gradually dilates. It turns out something like a hydraulic wedge.
In other words, the uterus itself rises, thereby pushing the fertilized egg down. Along with the fetus, amniotic fluid descends, rushing to thinner-walled segments, where the tension is weaker. This is how the unborn child moves towards the exit, and the cervix becomes not smooth.
Smoothing and dilation of the cervix
At that moment, when the muscle mass straightened the cervix, the uterus gradually smoothed out and expanded the birth canal, through which the child, along with the bladder of the lower part of the egg and amniotic fluid, was implanted down. This period is considered the longest and ranges from 6 to 16 hours. The cervix has three phases of opening:
- Latent - the cervix opens by 3-4 cm. Duration is 4-6 hours;
- Active - opening occurs by 1.5-2 cm in one hour. May increase up to 8 cm;
- Slow - the cervix opens by 1-1.5 cm in one hour. Reaches full opening up to 10-12 cm.
How the uterus opens before childbirth
When the cervix has reached a certain size of dilation, the amniotic sac bursts and water leaves, which has neither color nor odor. This is considered excellent performance because everything happened in a timely manner. Sometimes your water may break before contractions begin. In this case, it is called premature waters. If you are afraid of pain, you can ask the doctor to give you an anesthetic, but this is not always possible, as it depends on the general condition of the fetus and the woman in labor. After the fetus is delivered, that is, after childbirth, the obstetrician must first remove the amniotic fluid and cleanse the cervix and uterus of all unnecessary things.
Natural dilatation of the cervix before childbirth
The uterus itself is composed of smooth muscle, and the cervix includes connective tissue, collagen and elastic fibers, and smooth muscle cells. When a woman is pregnant, some of the muscle fibers in her cervix are replaced with connective tissue. This is due to their greater elasticity and ability to stretch. With an excess of collagen fibers, the cervix becomes shorter and the internal os widens.
During normal pregnancy, the cervix remains long (approximately 35-45 mm). This is a mechanism for protecting the body from miscarriage and infection. During normal pregnancy, the structure and length of the cervix begins to change only a few weeks before the expected date of birth.
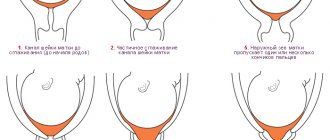
The dilatation of the cervix indicates the onset of labor. Obstetricians measure it with their fingers during an internal examination. Full dilatation of the cervix corresponds to five fingers of the obstetrician or ten centimeters. Just before childbirth, the cervix becomes shorter and is approximately one centimeter in length.
Before childbirth, the cervix does not dilate, reasons
If, on the eve of childbirth, a woman’s cervix does not naturally dilate, this may indicate that the birth canal is not sufficiently prepared for the passage of the child.
The cause of this condition may be insufficiently active contractions or various neuro-reflex pathologies that provoke excessive contraction of the smooth muscles of the cervix.
A healthy natural birth is accompanied by dilatation of the cervix sufficient for the unhindered release of the child into the big world. If during childbirth the uterus remains closed, then the specialist delivering the baby must immediately begin all the necessary manipulations to stimulate the readiness of the reproductive organs for the upcoming birth.
However, such manipulations must be carried out exclusively under the supervision of a specialist, otherwise the life and health of the child may be endangered. Only a specialized specialist can prepare the cervix for the upcoming birth; this process is called uterine stimulation, and if it starts in a timely manner, labor, as a rule, proceeds without problems. Such manipulations are recommended to be carried out after the fortieth week of pregnancy, since during this period the child is already fully formed and ready for life outside the mother’s body, and the placenta is going through the aging stage.
Premature cervical dilatation during pregnancy
Premature dilation of the cervix or isthmic-cervical insufficiency is a pathological condition that can lead to termination of pregnancy in the second and third trimesters of pregnancy. With this pathology, the cervix begins to shorten, becomes softer and thinner, losing the ability to hold the fetus in the uterus for up to 36 weeks. Due to this pathology, about 20% of miscarriages occur in the second trimester of pregnancy.
Causes of premature cervical dilatation during pregnancy:
- Organic. They are the result of previous injuries to the cervix during a previous birth, abortion, miscarriage, or treatment of certain diseases, for example, erosion using the cauterization method. The injury leads to the replacement of muscle tissue in the cervix with scar tissue, which is less elastic in its properties and is unable to hold the fetus inside the uterus.
- Functional. It occurs due to an imbalance in the ratio of muscle and connective tissue in the cervix or due to disruptions in its hormonal regulation. As a result, the cervix becomes too susceptible to fetal pressure and begins to dilate as it enlarges. It occurs in women with ovarian dysfunction or may be congenital.
Symptoms of premature cervical dilatation during pregnancy.
The following symptoms may be a signal of premature dilatation of the cervix during pregnancy:
- nagging or sharp pain in the lower abdomen in the early stages;
- sometimes the pain is accompanied by diarrhea;
- nausea.
These symptoms should be a reason to consult a doctor. An accurate diagnosis can be made by examining the cervix in a speculum. In addition, ultrasound helps to diagnose pathology in the early stages, where you can see the expansion of the internal pharynx.
Premature opening of the internal os during pregnancy, causes and treatment.
Causes and characteristics of isthmic-cervical insufficiency during pregnancy, prevention of premature birth.
Main stages of prenatal activity
First of all, there is no need to panic, since the first birth does not occur quickly. It’s as if nature itself, aware of the pregnant woman’s fears, makes it possible to slowly get acquainted with the sensations. First of all, it should be noted the frequent contractions, which gradually intensify. This manifests itself in compression and tension of the uterus, which needs to be smoothed out. Such sensations accompanied the woman during the last months of pregnancy, but were quite rare. Main features:
- Nagging pain in the lower abdomen;
- Severe lumbar pain;
- Sharp pain in the abdomen;
- Labored breathing.
When contractions are duplicated every five minutes, it’s time to go to the maternity hospital.
Treatment of premature cervical dilatation
Treatment can be surgical or conservative.
Surgical treatment consists of circular suturing of the cervix. The operation is performed in a hospital under local anesthesia. Contraindications to such an operation are: infections of the genitourinary system, increased tone of the uterus, uterine bleeding, etc.
A conservative method is the use of a pessary - a special device made of silicone or plastic that narrows the cervix and prevents it from opening. The pessary is placed on the cervix, its edges rest against the walls of the vagina, preventing the ring from moving. The plastic pessary also redistributes fetal pressure. This treatment method can be combined with surgery.
Our obstetric unloading pessaries are an effective measure for the prevention and treatment of ICI. The products have passed all the necessary clinical tests and have all the necessary certificates and permits.
The first stage of labor is the opening and effacement of the cervix
As soon as contractions become rhythmic, they repeat at least 5 times in 1 hour, that is, they repeat every 10 to 12 minutes, and then more often. Their rhythm increases, the duration of the contraction increases from 20 seconds to 35 - 45 - 60 seconds, and the pause decreases to 3 - 4 minutes, they say that the first stage of labor has begun.
In the first stage of labor, there is a gradual smoothing of the cervix, opening of the external and internal pharynx of the cervical canal to a degree sufficient to expel the fetus from the uterine cavity
1. The opening and smoothing of the cervix is carried out under the influence of labor contractions. In the muscles of the cervix occurs:
- Contraction
is
the contraction of muscle fibers. - Retraction is the displacement of muscle fibers. The muscle fibers move, move into the adjacent layer and shorten. As a result, the wall of the uterus thickens, and the lower uterine segment becomes thinner and stretched, which leads to shortening, smoothing of the cervix and opening of the uterine pharynx.
- Distraction - contracting muscle fibers of the uterus pull the circular muscles of the cervix to the sides and upwards, which also contributes to the opening of the uterine pharynx.
2. The dilatation of the cervix is facilitated by the movement of amniotic fluid towards the cervical canal.
With each contraction, the muscles of the uterus exert pressure on the contents of the fertilized egg, mainly on the amniotic fluid. Due to uniform pressure from the fundus of the uterus, amniotic fluid, according to the laws of hydraulics, rushes towards the lower segment of the uterus. Here, in the center of the lower section of the fetal sac, the internal os of the cervical canal is located, where there is no resistance. Amniotic fluid rushes to the internal os and, under their pressure, the lower pole of the fertilized egg is introduced into the internal os of the cervical canal. This part of the membranes of the lower pole of the fertilized egg is called the amniotic sac.
During contractions, the bladder stretches (fills up) and penetrates more and more into the cervical canal, expanding it.
- The opening of the cervix is also facilitated by the presenting part of the fetus moving through the birth canal.
The cervix consists of cavernous spaces filled with blood. The presenting part displaces blood from these spaces, the neck becomes thinner and gradually disappears, and the pharynx opens.
The opening increases by 2 - 4 - 6 cm, etc. until full opening - 10 -12 cm.
The process of dilation of the cervix is different for primiparous and multiparous women.
In primigravidas, before the start of the first stage of labor, the external and internal os are closed. With the beginning of the first stage of labor, the internal os opens, then the cervical canal gradually expands, which takes the shape of a funnel, tapering downward. As the canal expands, the cervix shortens and finally flattens out completely. Only the outer pharynx remains closed. Next, the edges of the external pharynx become thinner, and it begins to open with each contraction.
more and more until it opens completely (up to 1-12 cm).
The dynamics of opening is 1 cm per hour.
In multiparous women, already at the end of pregnancy, the external pharynx is dilated by 1.5 - 2 cm. During the period of dilation, the external and internal pharynx open simultaneously and the cervix is smoothed. The dynamics of opening is 2 cm per 1 hour, i.e. 2 times faster.
Contact belt.
During each contraction, amniotic fluid rushes to the lower pole of the fertilized egg; the amniotic sac is stretched (filled) and inserted into the pharynx. After the end of the contraction, the water partially moves upward, the tension of the fetal bladder weakens. Free movement of amniotic fluid occurs as long as the presenting part is mobile above the entrance to the pelvis. When the head descends, it comes into contact with the lower segment of the uterus on all sides and presses this area of the uterine wall against the entrance to the pelvis.
The place where the head is covered by the walls of the lower uterine segment is called the contact zone.
It divides the amniotic fluid not anteriorly and posteriorly.
The anterior waters are located below the contact zone, the posterior waters are located above. The water is distributed as follows: front water - 200 - 250 ml, rear water - up to 1.5 liters. During contractions, the anterior segment of the amniotic sac tenses, and the “wedge” plunges into the expanding cervix. Such a fetal bladder is called functioning .
Sometimes there is little front water. They cannot facilitate the opening of the cervix, but, on the contrary, by stretching on the head, they prevent the advancement of the head. Such a fetal bladder is called flat
-
not functioning.
By preventing the advancement of the head, it helps to lengthen the period of dilatation, and, consequently, the duration of labor. Such a fetal bladder is opened. When the anterior waters outside the contraction do not leave due to the contact zone, they say that this amniotic sac is “ready to rupture.”
Rupture of the membranes.
Rupture of the membranes usually occurs at the end of the first stage of labor, that is, at full dilation, when the function of the membranes is completed.
This is the timely release of amniotic fluid.
For some women in labor, water does not pour out in a timely manner:
- Before the onset of labor - premature.
- Before full disclosure - early. Early rupture of the membranes (as well as premature rupture) leads to complete rupture of water from the uterus -
“dry birth”, which is accompanied by a number of complications, sometimes severe:
1. rupture of amniotic fluid before the formation of the contact zone can lead to the loss of umbilical cord loops and small parts of the fetus
(arms or legs), which complicates the course of labor and poses a threat to the life of the fetus;
2. the cervix dilates more slowly;
3. the first stage of labor is lengthened. if the anhydrous period exceeds 12 hours, they speak of a long anhydrous period, which poses a threat of the development of an intrauterine infection.
- If the membranes are very dense, the amniotic sac may not open and then the baby is born “in a shirt” - in the membranes. This is a delayed rupture of the membranes. A child at birth may choke on water. Therefore, such a fetal bladder is opened in advance, i.e. is performed .
Biomechanism of childbirth.
The bony pelvis is characterized by unequal size of its walls and dimensions in individual planes. The walls of the small pelvis are uneven: the symphysis is much shorter than the sacrum, the inner surface of the latter is concave. The shape of the small pelvis at different levels is not the same: the inlet has a transversely elongated shape, the pelvic cavity is round, the outlet is an oval, elongated in the anteroposterior direction.
The soft tissues of the birth canal include the expanded lower uterine segment, vagina, parietal muscles and pelvic floor.
The diameter of the birth tube corresponds to the diameter of the emerging head and body of the fetus. This tube, which is a continuation of the bone canal, is not straight, it goes obliquely, bending in the form of an arc. The lower edge of the birth canal, the formations of the vulvar ring, also lengthens and sharply bends anteriorly (upward). Therefore, the pelvic wire line has the shape of a curve: in the bone canal it goes down almost straight (through the centers of straight dimensions), in the pelvic floor it bends and goes anteriorly (up).
Due to these features of the birth canal, the head cannot pass through the birth canal in a straight line without making turns. Simultaneously with translational movements along the axis of the birth canal, the fetus, especially the head, makes a series of movements. It performs translational movements, rotations around the longitudinal axis and rotation around the transverse axis - flexion and extension.