Causes
Among the most common causes of ovarian cysts are dysregulation of the menstrual cycle, lack of normal ovulation, and disruption of follicle maturation processes.
Endometrioid cysts are an external form of endometriosis, a systemic hormone-dependent disease. The appearance of teratomas is based on disturbances at the stages of embryogenesis; these types of tumors are always congenital and can occur in both ovaries.
Extragenital causes include dysfunction of the thyroid gland, obesity, prolonged stress and emotional stress, poor lifestyle, and frequent abortions.
Preparation for surgical treatment
Ovarian cyst is a fairly common pathology in women of all ages. Very often, such a formation can greatly increase in size, causing serious complications.
There are cysts that are not dangerous to health and resolve over time without medical help, but in some cases they can pose a threat even to a woman’s life and provoke the development of persistent infertility, so specialists may prescribe removal of an ovarian cyst.
The choice of method used to remove the tumor will depend on the likelihood of complications, the age of the patient, her general health, the size of the tumor, etc.
Briefly about the cyst
A cyst is a benign formation that can affect the structure of the ovaries and disrupt their functioning. The causes of tumors can be the following:
- hormonal imbalance;
- diseases and injuries of the genital organs;
- disorders at the gene level;
- congenital pathology in the organs of the reproductive system.
At the initial stages of cyst formation, symptoms may be completely absent, but as the tumor increases in size, a woman may suddenly experience pain in the lower abdomen during sex and physical activity, urination becomes more frequent, nausea and vomiting occur, and the temperature rises to 39°C.
There are several types of cysts on the ovaries. Functional (follicular, luteal) can resolve on their own, provided that the cause that caused them is eliminated.
Most often they are formed against the background of hormonal imbalance that occurs during the menstrual cycle. As soon as the disturbances are eliminated, the tumor begins to regress.
In rare cases, non-surgical treatment of an ovarian cyst may be necessary; most often it resolves on its own.
If an endometrioid, dermoid or paraovarian cyst is diagnosed, the only treatment option in this case is surgery. Surgery is also prescribed when a cyst-like tumor, such as a teratoma, fibroma or cystadenoma, is detected on the ovaries. It is impossible to stop the growth of such tumors with medications.
Since neoplasms on the female reproductive glands occur in most women, many are interested in the completely natural question of in what cases it is necessary to remove a cyst, and when this should not be done.
Often, if the size of the cyst is small, it appears in a single copy, and especially if this happened during menopause, then a wait-and-see approach is chosen.
For several menstrual cycles in a row, the neoplasm is treated with hormonal drugs and vitamins, and medications are also prescribed to eliminate the accompanying symptoms. Additionally, suppositories for cysts may be prescribed.
If after 3 menstrual cycles the tumor resolves on its own, then surgery is not necessary. If there is no improvement or the size of the cyst, on the contrary, increases, surgical intervention is performed.
Let's consider other indications for surgery to remove a cyst.
If a woman is diagnosed with a cyst on the gonads, only the attending physician can determine the method of eliminating the tumor - conservative treatment or surgery, taking into account many factors, ranging from the general health of the patient to the size of the tumor. We list the main indications for surgery:
- the size for surgery of a tumor is its diameter of 3 centimeters or more;
- if there is no positive dynamics with drug treatment of the cyst, surgery is necessary;
- there are suspicions of the presence of malignant processes in the neoplasm;
- if the cyst has a long stalk, surgery is performed to prevent it from torsion;
- a woman experiences constant abdominal pain caused by the growth of a tumor;
- if the functioning of nearby organs, such as the intestines, bladder, is disrupted, they may be affected by an increasing tumor;
- if the neoplasm disrupts blood circulation in the ovary;
- with polycystic disease;
- direct indications for emergency surgery to remove a cyst may be signs of complications (rupture of the tumor, torsion of the leg, abdominal bleeding, apoplexy of the gonad), such as severe abdominal pain, bloating, fever and fainting.
There are various ways to remove cysts on the ovaries, the choice of a specific technique will depend on the size of the tumor, its type and the presence of complications, and experts also take into account the woman’s age. If the patient still plans to have children, the cyst is removed using the most gentle methods while preserving reproductive function. Surgical intervention can be of several types:
- cystectomy – the tumor is removed, but the ovary remains functional, after which the woman is still able to bear offspring. This operation is performed when benign cysts with a diameter of 3-5 cm are detected;
- wedge resection - the tumor is excised along with a small area of ovarian tissue. This is a more traumatic type of operation; it is prescribed for a wide base of the tumor, when it grows to the tissues of the genital organ;
- oophorectomy - during such an operation the ovary is completely removed, it is prescribed for ovarian apoplexy, for suppuration or twisting of the tumor, that is, if there is a threat of peritonitis;
- adnexectomy - during the intervention, the ovary is removed along with the fallopian tube, prescribed when the malignant nature of the tumor is confirmed.
To determine the presence of cancer cells, an ovarian biopsy is performed using diagnostic laparoscopy, and specialists send the selected material for histological examination.
There are two methods to remove a cyst:
- laparotomy or abdominal surgery to remove an ovarian cyst;
- Laparoscopy of a cyst is a more gentle method of eliminating a tumor, one of the varieties of which is laser removal of the tumor.
Laparotomy
During laparotomy, a layer-by-layer dissection of the abdominal tissue is performed and the cystic capsule is excised along with the affected tissues and organs as necessary. This type of operation is prescribed in the following situations:
- the tumor ruptured and its contents entered the abdominal cavity;
- adhesions were detected;
- malignant tissue degeneration has been confirmed;
- suppuration began;
- if the cystic capsule is huge.
During such an operation, it is possible not only to remove the tumor itself, but also to cut out endometrioid lesions, adhesions and clean purulent areas of tissue.
For the operation, the patient needs to stay in a hospital for 5-7 days. You can begin active activities no earlier than after 1.5-2 months.
To avoid complications, it is necessary to follow all recommendations of the postoperative period.
This method is used in extreme cases because it is very traumatic, is performed under general anesthesia and requires a long recovery time. If the operation is performed correctly, then there should be no complications, but to prevent relapse, hormonal therapy, immunostimulants, vitamins and physical therapy may be prescribed.
Laparoscopy
During laparoscopic cyst removal, local anesthesia is used, and the risk of postoperative complications is minimal, the patient quickly recovers and returns to an active life.
The operation goes like this: 3-4 punctures are made in the abdominal cavity, into which a micro-video camera and instruments are inserted, and a special gas is pumped inside, which lifts the abdominal walls, improving visibility and providing mobility to the instruments.
This technique is used in the following cases:
- the cystic formation is small in size;
- no suppuration;
- if there is 1 tumor or there are several but small formations;
- the neoplasm affected the superficial layers of the ovary, but did not affect its functionality.
Specialists monitor the progress of the operation on the monitor screen, so the surgeon can assess the condition of the ovaries and other organs, then the cystic capsule is opened, the contents are removed using special instruments and the capsule itself is excised. Next, the abdominal cavity is disinfected, gas is removed from it, drainage is installed and sutures are placed at the puncture points.
Sutures are removed 6-7 days after surgery. To prevent the development of inflammatory processes, antibiotics and painkillers may be prescribed to relieve pain.
Laser technique
Laser removal of a cystic tumor on the ovary is very similar to laparoscopy, but the tumor is excised not with a scalpel, but with a laser beam. The surgeon opens the capsule and removes it to healthy tissue.
Removing an ovarian cyst with a laser helps prevent bleeding during the operation, since the laser immediately cauterizes the problem areas. This method is considered the most promising among other laparoscopic techniques.
If a cystic formation is detected in a pregnant woman, the attending physician will initially prescribe regular ultrasounds to monitor the dynamics of tumor development. Additionally, light drug treatment can be selected that will not be dangerous for the patient and the fetus.
If drug treatment is ineffective and the pregnant woman’s condition worsens, surgery is prescribed, which is most often performed laparoscopically. Laparotomy is prescribed for very large tumors and in the most extreme cases, since this technique is dangerous for both mother and baby.
If a woman is diagnosed with a cystic tumor in the gonads and is scheduled to have this tumor removed, she must first prepare for surgery. A fluorography and cardiogram should be done, as well as a number of additional studies. Preoperative tests may include the following:
- blood group and Rh factor;
- general and biochemical analysis of urine and blood;
- tests for blood clotting ability;
- examination for the presence of infectious diseases.
Indications for laparotomy
Laparotomy is required in the following cases:
- large volume of cystic growth;
- the pathology is accompanied by purulent formation;
- the cyst is localized in the tissues of the organ (deep) and negatively affects the functions;
- complicated cysts - torsion of the legs or violation of the integrity of the capsule;
- adhesions;
- oncologic changes.
Several advantages:
- The surgeon has the opportunity to carefully examine the pelvic organs, tissue and lymph nodes in order to rule out various complications, including cancerous tumors.
- The cyst can be completely excised without compromising its integrity. This intervention does not allow pus or fluid to enter.
- If during the operation the specialist discovers uterine fibroids, it can also be removed without the risk of bleeding.
Important! With timely treatment of ovarian pathologies, complications that can lead to complete removal of the organ can be avoided.
Symptoms
In some cases, patients complain of nagging pain in the lower abdomen, pain during sexual intercourse, and atypical intermenstrual bleeding.
If the cyst grows to a very large size, it can put pressure on the rectum or bladder and lead to difficulty defecating and urinating.
- Menstrual irregularities;
- Periodic nagging pain in the lower abdomen;
- Dysuric disorders;
- Disruption of the digestive system;
- Infertility.
Contraindications
Before abdominal surgery and laparotomy, the woman is examined to identify direct or indirect contraindications to their implementation. Surgical interventions are strictly prohibited for:
- stroke, heart attack, other serious pathologies of the cardiovascular system,
- blood diseases associated with blood clotting disorders,
- any chronic diseases in the acute stage,
- decompensated diabetes mellitus.
In the presence of acute chronic or infectious conditions, abdominal surgery is postponed until recovery or stabilization of the condition.
Diagnostics
Smaller tumors are best diagnosed with routine ultrasound. This method allows you to evaluate the exact size, structure and expected nature of the formation.
The doctor also conducts a Doppler examination of the vessels feeding the cyst. Additional instrumental methods are computed magnetic resonance imaging.
These studies may be prescribed if the location is atypical or difficult to visualize on ultrasound.
From laboratory tests, it is necessary to determine the tumor markers CA-125 and HE4. They help indirectly assess the benign nature of the tumor.
Verification of the diagnosis of a large cyst is made on the basis of the medical history, life history, complaints, objective examination, gynecological examination and data from additional research methods:
- Ultrasound examination of the pelvic organs (abdominal and transvaginal method);
- Puncture of the posterior vaginal fornix;
- CT and MRI diagnostics;
- Clinical blood and urine tests;
- Diagnostic laparoscopy;
- Blood test for tumor markers CA-125.
Treatment of cystic formations depends entirely on the type, size, shape and can be either conservative or surgical. With conservative therapy, a woman is prescribed hormonal, anti-inflammatory and antibacterial therapy. The woman is advised to undergo physiotherapeutic procedures. Surgical treatment is indicated for large tumors or sudden complications (torsion of the cyst stalk and apoplexy of the ovarian cyst).
Yusupov Hospital is a multidisciplinary center that provides various medical services based on European quality standards. The professional team of doctors at the oncology clinic are specialists with extensive practical experience. Modern diagnostic equipment within the walls of the hospital, as well as our own laboratory, allows our specialists to conduct any research in the shortest possible time. To make an appointment, call by phone.
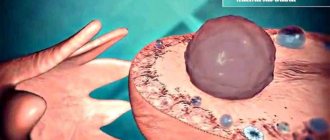
Ovarian cyst: sizes and norms
The most important part of a woman’s reproductive system is the ovaries, in which the development of eggs necessary for conception occurs.
One of the most common pathologies of these paired organs is a cyst. According to statistics, various cystic formations are diagnosed in more than 40% of women.
Often the disease is asymptomatic and is detected during ultrasound diagnostics during a routine visit to the gynecologist.
Any ovarian cyst larger than 2 cm in diameter is considered potentially dangerous. Ovarian cysts range in size from 33 mm to over 20 cm in diameter.
Small functional formations up to 10 cm in diameter do not require surgical treatment. They often regress on their own within 1-3 months. A real danger to a woman’s health are large cysts, which can cause massive internal bleeding.
An ovarian cyst up to 5 cm remains within acceptable limits. They rarely show symptoms. Most often, gynecologists prescribe complex medications and limit themselves to regular monitoring over time.
Possible complications
After undergoing surgery, a woman may experience the development of various types of complications.
It should be remembered that any surgical intervention is characterized by the presence of risks and dangers.
More often than not, the surgeon’s skills influence the occurrence or absence of complications. The most common complications are:
- the appearance of adhesions;
- pain on the seams;
- if there is an infection under the stitches, inflammation develops;
- an unsuccessful operation may be accompanied by injuries to the intestines and other internal organs.
When is surgery to remove a cyst necessary?
An ovarian cyst is a benign tumor-like formation filled with fluid.
The pathology can make itself felt by menstrual irregularities and pain in the lower abdomen or remain asymptomatic.
Some ovarian tumors cause infertility and miscarriage, lead to compression of the pelvic organs and other serious complications.
Ultrasound is actively used in diagnosing pathology of the appendages. With ultrasound, it is important to determine the size of the ovarian cyst - as an indication for surgery. For additional diagnostics, MRI or CT is prescribed. After assessing all parameters, a treatment method is selected and the prognosis of the disease is determined.
It is important to understand what size an ovarian cyst can be, and at what size surgery is indicated. In some cases, this parameter is the key in deciding on surgical intervention.
In gynecology there is no single classification based on the size of tumors. In diagnosing pathology, size matters, but other parameters are also taken into account. First of all, it is important for the doctor to understand which type of cyst has formed in the uterine appendages:
- Follicular. Education occurs only in the first phase of the cycle. A cavity appears from a follicle that has not undergone ovulation. Conception during this cycle becomes impossible. Can reach a size of 10-15 cm. Prone to spontaneous regression within 1-3 months;
- Luteal. It is formed from the corpus luteum only after ovulation, in the second phase of the cycle. Often accompanies pregnancy. Capable of producing progesterone, which explains its clinical symptoms. It grows slowly and rarely exceeds 6-8 cm in diameter. May disappear spontaneously within 3 months;
- Dermoid. It is a congenital pathology and occurs when intrauterine development is disrupted. Inside it contains embryonic tissues - bones, legs, hair, fat. It grows slowly, but can reach a very large size - up to 20 cm or more;
- Paraovarian. Appears next to the ovary and is not directly connected to it. It is considered a congenital pathology. Can grow up to 15 cm or more;
- Endometrioid. Occurs when cells from the mucous layer of the uterus grow in the ovarian tissue. Can be detected on both appendages. This is usually a small cavity - up to 4-6 cm in diameter. Rarely reaches a size of 10 cm or more;
- Serous. The many options for the development of this pathology do not allow us to predict its growth rate.
In gynecology, there is no such thing as the normal size of an ovarian cyst. We can talk about the norm only in relation to functional formations:
- A follicular cyst is a lesion 3 cm in diameter. A cavity measuring 2-3 cm may be a normal follicle that has reached the peak of its development;
- The corpus luteum cyst should be between 2.5-3 cm in diameter. If the value is lower, there is no talk about pathology.
Conventionally, ovarian formations can be divided by size as follows:
- Small – up to 3-4 cm in diameter;
- Medium – 3-6 cm;
- Large – 6-10 cm;
- Giant - 10-12 cm or more.
The permissible size of an ovarian cyst is primarily determined by its type. And if a follicular formation measuring 8-10 cm is not surprising, then the cavity arising from the corpus luteum rarely reaches such a diameter. Rapid growth is always an alarming symptom that requires special attention from a doctor and a solution to the issue of emergency surgery.
The size of the ovarian mass is determined by ultrasound. It is important to monitor changes in dynamics. If a once asymptomatic small formation has increased several times over the course of a year, you need to undergo additional examination: CT, MRI, laparoscopy, test for tumor markers.
As a rule, the size of an ovarian cyst and its dynamics are determined by ultrasound.
The size of the cyst affects the symptoms of the pathology. Small formations up to 30 mm in size (the size of a quail egg) usually do not manifest themselves. A woman may not know there is a problem until she has an ultrasound. Often we are talking about functional cysts that resolve safely without the use of medications.
A gynecological ultrasound is performed on the 5-7th day of the cycle (unless the doctor recommends otherwise). During examination, lesions ranging in size from 2-3 cm are clearly visible. Small formations are not always visible during ultrasound and are often indistinguishable from normal follicles.
Medium lesions measuring 3-6 cm (the size of a chicken egg) can manifest themselves with the following symptoms:
- Menstrual irregularities. With functional formations, there is a delay in menstruation, after which prolonged and heavy bleeding occurs. Endometrioma produces spotting before and after menstruation. Other cysts do not affect the menstrual cycle;
- Uterine bleeding is observed mainly against the background of endometrioma. This pathology is often combined with a hyperplastic process of the endometrium;
- Nagging pain in the lower abdomen is characteristic of any type of formation.
A sign of the presence of a cyst may be nagging pain in the ovarian area.
Large cysts are characterized by the following symptoms:
- Pressure on the pelvic organs leads to constipation, bloating and urination problems;
- Increase in size of the abdomen due to growth of formation.
On a note
The largest ovarian cyst was removed in 1991 in California from a 36-year-old woman. The formation weighed 137 kg. It reached this level in 2 years. Dr Catherine O'Hanlan, head of the surgical team, said the patient was afraid of the operation and did not see doctors for a long time. Removing the giant cyst took 6 hours.
In 2021, a complex operation was performed in Mexico to remove a cyst weighing 33 kg. The diameter of the formation was about 150 cm. Dr. Eric Hanson Viana, who performed the operation, points out that this is the only case in the history of medicine when a cyst of this size could be removed without pumping out fluid from it or damaging the capsule.
It is also useful to read: Regulon in the treatment of ovarian cysts
It is not completely known what size a particular cavity can grow - in a month or in a year. In gynecology, there are cases where a woman’s cyst has increased several times in just 10-12 months. On the contrary, it happens when the identified tumor practically does not grow, remaining approximately the same diameter for many years.
The growth of education is influenced by the following factors:
- Woman's age. Cysts begin to grow in adolescence due to hormonal changes. During menopause, some formations disappear. The appearance of a tumor in postmenopause is an alarming symptom that speaks in favor of malignant degeneration;
- Pregnancy. Some ovarian masses rapidly increase in size during gestation, while others shrink;
- Taking hormonal drugs. Gonadotropin-releasing hormone agonists, COCs, gestagens and some other drugs lead to regression of the lesion. Emergency contraception leads to the appearance of ovarian cysts;
- Abortions, miscarriages and traumatic births can cause the growth of ovarian tumors.
According to women, stressful situations can lead to an increase in tumor size, but no reliable evidence of this has been found.
It is believed that stress can cause tumor growth.
As the pathological focus grows, the risk of complications increases:
- Infertility. Hormonally active formations prevent ovulation and conception of a child. Large cysts, even those without hormonal activity, can compress the fallopian tubes and impair their patency, making fertilization impossible;
- Miscarriage. Lesions detected during pregnancy may continue to grow until delivery, interfering with the development of the fetus. It is possible that pregnancy may be terminated, the development of placental insufficiency, premature birth and other complications;
- Capsule rupture. The larger the cyst, the higher the risk of its rupture with hemorrhage into the ovary. If the capsule bursts, peritonitis may develop - inflammation of the peritoneum. The rupture of a large formation is accompanied by profuse blood loss, which is life-threatening for the woman;
- Torsion of the pedicle of the formation. Large cysts on a thin stalk can twist, which leads to ovarian necrosis;
- Chronic pelvic pain. The cyst itself cannot hurt, but as it grows, it stretches the ovarian capsule and compresses the pelvic organs, which threatens to cause discomfort.
During pregnancy, the growth of an ovarian cyst can lead to premature birth and other complications.
The size of the lesion does not affect the likelihood of malignancy. Often, when examined, a small lesion turns out to be cancer, while a large lesion turns out to be an exclusively benign tumor.
It is customary to operate on ovarian neoplasms if the size of the lesion is 5-6 cm or more. But the size of the cyst is not the only indication for surgical treatment. It is important to consider other factors:
- Woman's age. Detection of ovarian pathology during menopause is a reason for surgical intervention;
- Reproductive plans. Before pregnancy, it is recommended to remove ovarian tumors, especially if IVF is planned. During gestation, large cysts must also be removed as potentially dangerous to the development of the fetus;
- Growth rate. If the lesion rapidly enlarges, surgery is inevitable;
- Presence of complications. If the pedicle is torsed, the cyst becomes infected, or its capsule ruptures, emergency surgical intervention is indicated;
- Signs of malignancy. It is necessary to undergo surgery if tests for tumor markers are positive. Surgery is also indicated when symptoms of a malignant tumor are detected on ultrasound and MRI.
Tests for tumor markers help to accurately determine the type of tumor, which can serve as an indication for surgical intervention.
The size of the lesion is not a decisive factor for the operation. It is important to evaluate all available data in order to choose the optimal treatment strategy.
Observation is indicated only for functional formations - follicular and luteal cysts. It does not matter significantly what size the lesion is if the pathology was detected for the first time. The waiting period is 3 months. During this time, the functional cyst should resolve. If this does not happen, the formation must be removed.
In some cases, the doctor may recommend taking hormonal medications to speed up the regression of the lesion.
Organic cysts - dermoid, serous, paraovarian - can only be treated surgically. Observation is not indicated even with minimal lesion sizes. Such an education is not capable of regressing on its own.
What it is?
Operation
At its core, laparotomy is a cavity intervention, a radical method for solving many ovarian pathologies, including cysts.
The intervention consists of dissecting the tissues of the upper part of the peritoneum using classical types of surgical instruments.
Despite the fact that tissue trauma during this operation is greater than during laparoscopy, in some cases it is simply necessary to use laparotomy.
Laparotomy can be performed using the following techniques:
- Cystectomy - the cyst is removed by enucleation, while healthy tissue is not affected. The functions of the organ and the reproductive function are preserved.
- Resection is the removal of a tumor along with part of the affected organ. This intervention is carried out when the cyst is large, as well as when the pathological focus is deep.
- Ovariectomy - resection of the entire ovary and cysts on it.
- Adnexectomy – excision of a cystic formation, ovary and fallopian tube. This technique is used in cases of significant destruction of ovarian tissue, as well as in the possible development of cancerous tumors.
- Hysterectomy – removal of the ovary and uterus. Prescribed for oncology or at a high risk of developing an oncological process.
All these techniques have one goal - to eliminate ovarian pathologies. The choice of method remains with the doctor.
Bibliography
- ICD-10 (International Classification of Diseases)
- Yusupov Hospital
- Cherenkov V. G. Clinical oncology. — 3rd ed. - M.: Medical book, 2010. - 434 p. — ISBN 978-5-91894-002-0.
- Shirokorad V.I., Makhson A.N., Yadykov O.A. The state of oncourological care in Moscow // Oncourology. - 2013. - No. 4. - P. 10-13.
- Volosyanko M.I. Traditional and natural methods of preventing and treating cancer, Aquarium, 1994
- John Niederhuber, James Armitage, James Doroshow, Michael Kastan, Joel Tepper Abeloff's Clinical Oncology – 5th Edition, eMEDICAL BOOKS, 2013
Surgery to remove an ovarian cyst: types and postoperative period
Recovery after laparoscopy is almost painless. A woman may feel slight pain and discomfort in the lower abdomen, but her general condition is rarely affected.
You are allowed to get up after surgery the very next day; hospital stay usually does not exceed 7 days.
Abdominal surgery requires much longer rehabilitation. The postoperative period is accompanied by pain of varying intensity, requiring the administration of painkillers.
It also takes some time to restore independent urination and defecation. Women usually stay in the hospital for up to two weeks and sick leave is issued for a longer period than with laparoscopic surgery.
For a month, you should refrain from physical activity, sexual activity, and avoid going to baths and saunas.
It is advisable to prescribe a short course of hormonal therapy to give the ovaries a “rest” after surgery.
Unfortunately, there is always a risk of recurrence of cysts on the ovaries, so a woman needs to be regularly observed by a gynecologist, undergo routine ultrasound examinations, and maintain a healthy lifestyle.
The disease may occur without pronounced symptoms, or may be accompanied by pain in the pelvic organs, menstrual disorder and frequent urge to urinate.
The reason for the development of cystic formation is a hormonal imbalance in the body, in which the process of releasing an unfertilized egg from the body does not proceed correctly. The following factors may be prerequisites for the development of a cyst:
- diseases of the endocrine system;
- heredity;
- depressive states;
- starvation;
- incorrectly selected oral contraceptive regimen;
- history of early puberty;
- diseases that suppress fertility;
- multiple abortions;
- increased BMI (body mass index);
- infectious and inflammatory processes in the pelvic organs;
- irregular intimate life;
- early termination of lactation.
All cysts can be divided into two types:
- functional;
- abnormal.
Functional benign formation is temporary and goes away without outside intervention. An abnormal neoplasm requires treatment. At the initial stage of development, drug correction of the condition is used. In later stages and if complications occur, removal of the ovarian cyst is required.
Based on the characteristics of the cellular structure of the cyst and localization, several types of formations are distinguished:
- follicular (occur as a result of improper maturation of the follicle);
- yellow-bodied (develops due to an imbalance of estrogen in the body);
- dermoid (includes particles of germinal tissue);
- endometrioid (grow into the deep tissues of the ovary);
- serous (represent an epithelial capsule with serous contents);
- paraovarian (develop at the border of the fallopian tube and ovary);
- hormone-producing (such cysts generate their own hormones and often become malignant);
- mucinous (includes a mucous substance and can degenerate into a malignant tumor, causing peritonitis of the abdominal cavity).
Reviews from various sources
Elena 32 years old
During a caesarean section, a cyst on the right ovary was discovered and immediately removed. When the histology came back, it turned out that it was a malignant tumor. After 3 days, they operated on the oncology clinic and removed everything: the uterus, the ovaries. The operation went well. But for a month I was tormented by terrible hot flashes, they prescribed Klimonorm, which helped. We had several courses of chemotherapy, after which I lost a lot of weight. Now I live an almost full life, raising two daughters. One of the consequences was osteoporosis. I’m thinking of starting to take calcium, but overall I’ll survive)
Video: Removal of the uterus and ovaries and possible consequences
Removal of the uterus and possible consequences