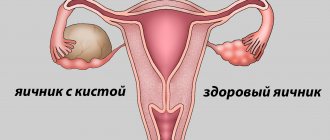
Unlike tumors of other organs, ovarian tumors are a variety of neoplasms. Most ovarian tumors are epithelial; tumors of the sex cord stroma and germ cell tumors are also found. The most common type of tumors are benign epithelial neoplasms, smooth-walled and papillary cystomas. One of the complications that occurs when an ovarian tumor develops is torsion of the tumor stalk. Torsion of the pedicle can occur in tumors with high mobility.
The Yusupov Hospital specializes in the treatment of malignant and benign tumors of various locations. The oncology department of the Yusupov Hospital uses all types of tumor diagnostics. The department is equipped with modern diagnostic equipment; patients can be treated in a hospital inpatient setting. Oncologists at the Yusupov Hospital treat ovarian tumor diseases. Diseases are treated with surgery, chemotherapy, radiation therapy, hormonal therapy, diet, and palliative therapy.
Definition
There is no need to explain what torsion is. Everyone understands on an intuitive level that this is a state in which various extended elements become entangled around one another. In this case, these elements are arteries and veins (vascular pedicle) that connect the ovarian cyst with the organ itself, nerves and lymphatic vessels.
In gynecology, there are two types of pedunculated cysts and ovarian formations: anatomical and surgical. In the first case, we are talking about obligatory formations: ovarian ligaments, various vessels, mesenteries. In the second case, a surgical pedicle is a twisted formation that sometimes pulls in intestinal loops, in some cases the fallopian tube, and sometimes even the omentum.
Source: Med-Explorer.ru
There is no doubt that such a secondary pathology is much more dangerous, since it leads to necrosis not only of the cyst itself or tumor formation, but also leads to impaired circulation in large organs and their necrosis.
If such a surgical pedicle resolves spontaneously after the occurrence of necrosis, this will lead, for example, to the escape of necrotic intestinal loops into the abdominal cavity, with the guaranteed development of peritonitis. In this case, it will be necessary to carry out extended surgical intervention with resection of necrotic intestinal loops.
But even if the twisted leg does not include other elements, its necrosis is still the cause of the development of peritonitis in almost 100% of cases, and requires urgent surgical intervention.
Etiology
As a rule, the causes of torsion are the presence of a formation in the ovary - a cyst, most often dermoid (due to its “heaviness”) or paraovarian (due to the presence of a thin stalk). Endometrial and malignant ovarian formations practically do not lead to torsion due to the pronounced adhesive process in the pelvis.
In childhood, in most cases, this pathological process is associated with an abnormal development of the ligamentous apparatus of the appendages, as a result of which the ovaries become more mobile, leading to torsions, sometimes bilateral and recurrent.
Isolated torsion of the fallopian tube is the rarest type of torsion, occurring in 1 in 1.5 million cases. According to foreign literature, the reason for this may be a history of tubal ligation, paratubar cysts located in the fimbrial region, hydro- or hematosalpinx.
Not the least role in the occurrence of torsion is played by the presence of adhesions in the pelvis, which, according to foreign studies, occurs in almost half of the patients.
- Diagnosis of acute pathology
- Hospitalization
- Laparoscopy
Causes
There are predisposing factors that contribute to the occurrence of such pedicle torsion. First of all, it is absolutely clear that the patient must have a corresponding cyst or tumor-like formation of a different nature, which has a rather long stalk connecting it to the main ovarian tissue.
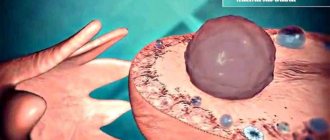
The cyst itself may have a greater ability to mobilize, or be free and moving within certain boundaries of its pedicle. But an even greater danger is posed by a cyst that has adhered to the peritoneum or to the surface of the ovary, and is itself already motionless, but at the same time it still has a free leg. It can grab any formation that has slipped inside and tighten it like a noose. A photo of a torsion of an ovarian cyst is presented below.
If such formations are discovered during routine gynecological examinations, and especially during ultrasound, it is recommended that they be removed routinely, before such disasters occur, using the usual laparoscopic method. But, unfortunately, it happens that many patients who neglect preventive and diagnostic procedures are diagnosed with the presence of these cysts through the development of complications. What predisposing factors contribute to torsion?
First of all, there is the movement factor. If the rotating torso suddenly stops, for example, during intense sideways turns, then this leads to the continued movement of the internal organs due to inertia. The pedicle of the cyst is stretched, and pathological torsion or pinching of other tissues occurs.
These are sports, dancing, physical labor. In addition to sports, such torsion is facilitated by a sharp turn even within the confines of bed, flatulence, diarrhea or irritable bowel syndrome, when its peristalsis increases. In some patients, this rise and torsion is facilitated by excessive overfilling of the bladder, pregnancy, and weakness of the abdominal wall muscles. Torsion of the pedicle of the right ovarian cyst occurs more often, due to its greater mobility and the characteristics of the adjacent structures.
Of course, rapid and acute twisting occurs most clearly. If the process is slow and proceeds with incomplete cessation of blood circulation, then, first of all, the venous outflow suffers, as a result, a plethora of the cyst develops, but arterial blood does not stop flowing.
As a result, necrosis and necrosis do not occur, and there is no risk of developing peritonitis. But this situation can lead to a significant increase in the cyst; at the beginning, pinpoint hemorrhages appear inside it, and then this cyst may rupture with bleeding into the abdominal cavity.
Bleeding, no matter how dangerous it may be, will not be accompanied by peritonitis in case of emergency hospitalization and urgent surgery. But if there is compression of the afferent arteries and acute development of the clinic, then the risk of peritonitis becomes very serious. What are the symptoms of ovarian cyst torsion in women?
Treatment and prevention of ovarian apoplexy
If medical care is provided on time, blood loss is insignificant and the type of disease is painful and not hemorrhagic, then conservative treatment is possible. But even in the absence of surgical treatment, taking medications, vitamins, physical therapy, etc. must occur in a hospital under 24-hour medical supervision. As complications in the future, a woman may develop adhesions in the pelvis, infertility and recurrent ovarian rupture.
The hemorrhagic form of the disease in case of untimely access to a medical facility can result in death. To avoid ovarian rupture, it is important to promptly treat emerging gynecological diseases, avoid hypothermia, and prevent infection with sexually transmitted infections (sex must be protected). It is important for every woman to undergo preventive examinations with a gynecologist: ideally every six months, but at least once a year.
Symptoms
The intensity and speed of development of symptoms depends on how completely and quickly the circulatory disorder occurs. For torsion of the pedicle of an ovarian cyst, it is characteristic that in the midst of complete health, and often after physical activity, very strong, cramping or paroxysmal pain occurs in the lower abdomen. Sometimes this pain radiates to the legs, to the lower back, and is localized on the side of the affected ovary.
Symptoms of ovarian cyst torsion include reflex intestinal paresis due to intense pain and possible bleeding, and retention of stool and gases. At the same time, due to extremely severe pain, there is “no way” to go to the toilet. Then nausea appears, possibly vomiting a small number of times, rarely multiple times, and after a few hours the body temperature rises.
This symptom may indicate the onset of necrosis and the addition of a secondary bacterial infection - the development of peritonitis. If we are talking about hemorrhage or rupture of the cyst as a result of torsion of the leg, then the patient will be more concerned about the symptoms of acute blood loss. These are increased heart rate and decreased blood pressure, pale skin and ringing in the ears, fainting, clammy sweat and tachycardia. Of course, partial torsion of the leg does not cause such a pronounced clinical picture.
What is ovarian torsion
Ovarian torsion is a pathological condition that is accompanied by disruption of blood supply processes caused by epididymal torsion and requires urgent surgical intervention. Pathology is detected in 3% of women of any age, however, its main share occurs in patients from seventeen to thirty years old. Sometimes the disease is diagnosed in adolescents, as well as in expectant mothers.
Torsion poses a danger to life and health. In adolescence, it occurs without an obvious clinical picture, so it is not always detected, which often becomes the reason for the involvement of nearby organs in the abnormal process and the development of inflammation.
Torsion of the pedicle of an ovarian tumor is explained by the inversion or bending of parts of the pedicle of an ovarian neoplasm. In this case, acute abdominal pain, vomiting, fever, and tension in the anterior abdominal wall occur. To identify pathology, the following are used: examination, ultrasound, laparoscopy. A confirmed diagnosis requires prompt adnexectomy or ovarian resection.
Torsion of the pedicle of the neoplasm
Diagnostics
A woman on her own will not be able to determine what caused it and what is happening in general. However, the symptoms of torsion of the pedicle of an ovarian cyst are a sign of a catastrophe in the abdominal cavity or in the pelvic organs, and oblige any woman to urgently call an ambulance.
During a gynecological examination, in typical cases, a tumor-like formation is clearly felt on the sides of the uterus, which can be very painful when displaced. Of course, this is determined by an enlarged cyst, if it has not ruptured. But such research is very often hampered by the developed protective tension of the abdominal muscles, which is called defence.
In the event that peritoneal irritation and symptoms of peritonitis intensify, this makes diagnosis even more difficult. Therefore, the main method of diagnosis is an ultrasound of the female genital organs and a dynamic study of red blood parameters.
An acute inflammatory process will be indicated by increasing leukocytosis up to 10 - 12 thousand, and even higher - up to 30-40. In patients, the ESR will steadily increase, the leukocyte count will shift to the left, and all this will be accompanied by an increase in fever and tachycardia.
But methods such as a general blood test should be used only for an auxiliary purpose. The main diagnostic method is ultrasound, or diagnostic laparoscopy with its transfer to urgent surgery using laparotomy.
Treatment
I would like the torsion of the pedicle of a cyst or tumor to be treated conservatively, but, unfortunately, this diagnosis almost always requires urgent surgery. And emergency care for torsion of the pedicle of an ovarian cyst is not at all connected with saving this cyst.
In the end, the body does not need this cyst. The thing is that the afferent blood vessels, which in 100% of cases are pinched, cause rapid and final necrosis of either a cyst or a tumor. And necrotic tissue necessarily undergoes microbial decay.
After all, protective cells are macrophages, neutrophils no longer have access to dead tissue, unlike microbes. And necrosis is always followed by either acute peritonitis, as a consequence of infection, or, in rare cases, fusion of the cyst with neighboring organs, which also leads to sluggish pelvioperitonitis.
Again, I would like to dispel doubts that surgery for torsion of an ovarian cyst is an easy matter and is performed laparoscopically in half an hour. In fact, unfortunately, this is not at all the case. Here we are talking about emergency gynecology, and doctors, taught by bitter experience, at the “acute abdomen” clinic are very often forced to transfer laparoscopy to abdominal surgery.
Many women, especially young women, for some reason believe that there is nothing terrible in this situation, you just need to “unscrew” this very leg, and everything will pass. There is perhaps no more dangerous misconception.
With this type of acute abdomen in gynecology, it is necessary not only to economically remove the cyst along with that very twisted neck, making one incision and applying a couple of stitches. First of all, it is necessary to perform an audit over a large area. In addition, sometimes this cyst turns out to be a malignant tumor that was not diagnosed during the “cold period”.
Doctors must examine the capsule of the cyst or tumor-like formation, evaluate its pedicle, the surface of the ovaries, and also carefully examine the pelvic and abdominal organs.
Indeed, with a long period that elapses between seeing a doctor and surgical intervention, symptoms of peritonitis, intestinal paresis, and accumulation of inflammatory exudate in the abdominal cavity are possible.
Also, with probable malignant degeneration of the cyst, it is possible to detect additional foci - metastases, and this will immediately require an expanded scope of surgical intervention according to the rules of ablastics, with possible removal of the ovaries and extirpation of the uterus.
In the case when a conventional horizontal Pfannenstiel incision is made, or a median laparotomy using a lower approach, the tumor or cyst is cut off in a different place, and not at all in the place where the torsion occurred. This is done in order to avoid the detachment of a blood clot, which formed at the narrowest point of the torsion when the blood flow was stopped, and can, if handled carelessly, enter the bloodstream, causing an embolism.
In a fairly large percentage of cases, a cyst or tumor-like formation fuses with the abdominal wall, as well as with neighboring organs, especially with delayed surgery. If the operation is performed laparoscopically, if access is insufficient, the cyst capsule can easily be ruptured, which will cause additional infection of the abdominal cavity, and in some cases, injury to the intestinal loops. Therefore, wide surgical access is required to remove a cyst or tumor from the abdominal cavity.
After this is done, if the cyst is “clean” and no signs of peritonitis and malignancy are detected, a crush clamp is applied to the pedicle of the cyst in a place closest to the normal ovarian tissue. After this, you can carefully unwind it, take it to the terminals and cross it.
The further stages of the operation are standard. Peritonization is performed, that is, the integrity of the peritoneum is restored, then possible bleeding is monitored and hemostasis is assessed. Then the abdominal cavity is toileted and, in case of timely surgery, before the symptoms of peritonitis, the abdominal cavity can be sutured on the first day of the development of symptoms.
If a long period of time has passed, and during the operation it is established that there is an effusion, a rupture of the capsule, there is a pronounced area of necrosis, or symptoms of an associated infection, then the abdominal cavity is not sutured. Then drainage is applied, the cavity is washed with antibiotic solutions, and further treatment is carried out in the intensive care unit with massive administration of antibacterial drugs intravenously, and, if indicated, intraperitoneally, according to the standards of peritonitis therapy.