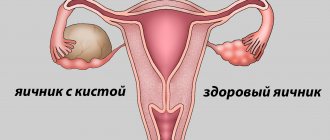
A woman should approach the issue of pregnancy planning very carefully and scrupulously. You should first visit a gynecologist and take directions for all the necessary tests. It is during this period that many people find out that the ovary is affected by a new formation. The cyst can be diagnosed on both sides, which significantly aggravates the situation.
The problem when an endometrioid ovarian cyst is identified and pregnancy, which does not occur as a result, is studied by specialists. The woman must undergo the prescribed treatment, adhering to the recommendations of specialists.
About endometrioid formation
Endometriosis is a pathological process in which active growth of the inner uterine layer of the endometrium occurs. As a result, blood clots form and parts of the uterine mucous tissue enter the organ, forming a cyst. It can be detected on one or both sides.
Women aged 25 to 40 years are most predisposed to this pathology. The risk of developing cystic formation increases when the first pregnancy occurs during this age period.
Experts do not have an exact answer as to what exactly provokes the appearance of education. Only common causes of endometrioid cysts have been identified:
- performing surgical intervention for gynecological indications;
- injuries of the reproductive system;
- retrograde menstruation;
- weakened immune system;
- disruptions in the functioning of the endocrine system;
- obesity;
- Navy;
- state of chronic stress.
Small formations do not make themselves felt. A woman faces unpleasant symptoms of the pathology when it reaches large sizes. During this period, the woman feels almost constant pain localized in the lower abdomen. The second characteristic sign of pathology is a disruption of the menstrual cycle. A woman periodically complains of:
- problems with stool;
- pain during sex;
- discomfort after active physical activity;
- pain when urinating;
- acceleration of hair growth. This is due to hormonal imbalance;
- the appearance of rashes on the face and body;
- discomfort in the intestines that occurs irregularly.
Should endometriosis be treated before planning a pregnancy?
Gynecologists have not yet reached a consensus on whether it is necessary to treat ovarian endometriosis in nulliparous women. Disputes arise regarding small cysts (up to 4 cm), which are not accompanied by significant clinical symptoms and do not lead to the development of complications. The opinion is expressed that such formations should not be touched. Proponents of this theory give the following arguments:
- Small endometrioma does not affect the ovarian reserve, does not interfere with ovulation and does not interfere with the conception of a child;
- If an endometrioid cyst is detected during pregnancy, it is not treated. So is it worth taking the risk and trying at all costs to eliminate education before conceiving a child?
- Hormonal treatment is not always effective and does not lead to complete regression of the lesion, but only helps to reduce it. After hormone withdrawal, the disease recurs;
- Surgical treatment can lead to the formation of adhesions and cause infertility. The risk is especially high after abdominal surgery, but also during laparoscopy there is a risk of developing adhesive disease.
A decision regarding surgical treatment should be made after discussing her reproductive plans with the patient.
There is another opinion, according to which endometrioid cysts should be removed before conceiving a child. Supporters of this version give their arguments:
- Endometrioma prevents the conception of a child and is one of the key causes of infertility in women;
- It is impossible to predict how a cyst will behave during pregnancy. As the formation grows, complications may develop, including termination of pregnancy.
The final decision is made individually, taking into account all known factors:
- State of the reproductive system. If a woman cannot conceive a child within a year, and no other significant causes of infertility have been identified, the cyst must be removed;
- Education size. Surgical treatment is recommended for lesions larger than 4 cm;
- Presence of symptoms. Severe menstrual irregularities and chronic pain in the pelvic area cannot be ignored;
- Woman's age. After 40 years, the likelihood of pregnancy decreases. Treatment of a cyst can take up to two years (including the recovery period after surgery). If there is a chance of spontaneous pregnancy, you can do without preliminary therapy.
When choosing a treatment method, it is worth taking into account all the individual characteristics of the course of the disease.
Indications for treatment:
- The size of the cyst is more than 4 cm;
- The presence of severe clinical symptoms;
- Development of complications associated with tumor growth;
- Suspicion of tumor malignancy.
The choice of treatment method is determined after the examination.
Compatibility with pregnancy
Pregnancy with an endometriotic ovarian cyst is quite problematic. Often the pathology becomes the cause of female infertility. If the formation was diagnosed already during pregnancy, the doctor continues to monitor it throughout the entire period of gestation.
A small formation does not affect the pregnancy process and the developing fetus. A woman with a similar diagnosis is at risk. A cyst can cause a miscarriage.
During pregnancy, the formation may resolve on its own. This is possible due to hormonal changes characteristic of this period. In some cases, the cyst begins to grow at this time.
If the cyst was diagnosed at the planning stage, it is removed. After this, the chances of conception increase significantly. Many women, having learned about the emerging education, insist on IVF. The procedure will not end positively. If the embryo attaches to the walls of the uterus, there remains a high risk of miscarriage.
Pregnancy with an endometrioid ovarian cyst is possible in some cases. This occurs rarely, provided there is a small number of atypical endometrial cells and the initial stage of development of the formation.
How does an endometrioid cyst prevent the development of pregnancy?
How to get pregnant with an endometrioid cyst on the ovary? An endometrial tumor is considered the most dangerous for the reproductive functioning of the female body. This is due to the fact that due to the peculiarities of tumor formation, a large number of adhesions often appear in the fallopian tubes, which prevent the birth of a new life.
After attaching to the ovaries, the capsule of the “chocolate” tumor begins to gradually grow, acquiring new layers of tissue and cells with each menstruation. Due to the fact that during the process of ovulation and menstruation, an increased flow of blood enters the ovaries, the cyst in the ovary quickly increases in size. Symptoms of the pathogenic influence of the cyst on the body can appear within a few months.
Diagnosis during pregnancy
A woman who is registered with a gynecologist during pregnancy is required to undergo regular examinations and undergo appropriate tests.
Suspicion of the development of a cystic formation of the ovary may arise during an interview and examination in a gynecological chair. To confirm the preliminary diagnosis, additional examinations are prescribed:
- Ultrasound with which you can visualize the formation and its size;
- biochemical blood test to determine hormone levels;
- blood test for ovarian tumor markers;
- CT scan to clarify the location of the cyst.
Based on the data obtained during diagnostic examinations, the doctor can confirm or refute the preliminary diagnosis.
Treatment before or during pregnancy
The chosen method of therapy directly depends on when the formation was detected. If the diagnosis is confirmed before planning a pregnancy, the doctor recommends removing it surgically.
The drug method cannot be considered the main therapy - it is an auxiliary method that prevents the growth of the cyst. Unfortunately, women often refuse surgery, preferring to take pills. As a result, this may worsen the current situation.
The most effective way is to listen to your doctor and agree to laparoscopy. This is the most gentle method that allows you to completely remove the formation. After the procedure, the woman recovers within 5 days. This is another advantage of the proposed method. After the manipulations, a recovery course is prescribed, which includes taking hormonal medications. After successful rehabilitation, we can talk about possible conception and bearing a healthy child.
If pregnancy occurs with an endometrioid ovarian cyst, the treatment regimen is strikingly different. The doctor observes the growth of education. If the cyst is small in size, there is no threat to the fetus. Changes in a woman’s hormonal levels during pregnancy can cause the lump to resolve on its own. In rare cases, the gynecologist additionally prescribes hormonal medications in a dosage that is safe for the child. If the cyst capsule ruptures, removal is required. Laparoscopy can only be performed in the 2nd trimester.
Childbirth with an ovarian cyst
Only your attending physician can accurately answer the question of whether it is possible to give birth with a cyst, since everything depends on the type of cyst, its size, symptoms, and the general condition of the pregnant woman. During childbirth, a cystic formation in the ovary can break through, then there is a threat of infection and the development of peritonitis. If surgery is necessary according to indications, a caesarean section can also be performed, during which the cyst is removed; in this case, it is usually impossible to give birth naturally.
Since during pregnancy there are many subtleties of treatment, as well as the risk of its termination for many reasons, we recommend that all women planning a pregnancy undergo examination and treatment of diseases at the stage of planning a child.
It is advisable to consult with several doctors, since medical practice is extensive, it may differ among doctors, and in order to take certain actions, it is necessary that a specific situation be studied comprehensively.
Pregnancy after cyst surgery
A woman of reproductive age who is faced with surgery and removal of a tumor may worry about the possibility of conception. Gynecological practice shows that if the rehabilitation period is successfully completed, pregnancy after removal of an endometrioid ovarian cyst occurs in the vast majority of women. There are general recommendations for those who are going to carry and give birth to a healthy child:
- During the rehabilitation period and in the future, you need to actively move so that adhesions do not form. The woman should get up 2-3 hours after laparoscopy. The adhesions of the fallopian tubes often become an obstacle to conception;
- You should strictly follow the doctor’s recommendations, without refusing prescribed medications or taking medications yourself;
- You should balance your diet, enriching it with healthy vitamins and minerals. Products that provoke fermentation should be excluded. Most of the menu should be liquid fresh dishes;
- the woman must be familiar with and follow all wound care recommendations.
Many people need psychological help. This will eliminate concerns in the future about the impossibility of conceiving or bearing a child.
Having heard the diagnosis of an endometrioid cyst, a woman should be prepared to follow the doctor’s instructions, possible surgery and the recovery period. A competent attitude towards yourself and promptly contacting a specialist with a problem will help you maintain reproductive health and become a happy mother of a healthy child in the future.
endometrioid cyst of the left ovary and pregnancy
So, I am 33 years old, in October I will be 34. We lived with our common-law husband for 3 years, and in 2021 we decided to formalize the relationship. There was a wedding in May, planning began somewhere in September 2021. Back at the end of 2015, I thought that it was getting close to the wedding, I needed to check my body. At that time, the ultrasound did not find anything other than a follicular cyst, although of impressive size, 4*5 cm in the PU. I visited mammologists and others with normal results. We observed 3 cycles and there was regression. With that I calmed down. In the same 2016, my husband and I’s brothers/sisters got married together with us, with a difference of + 1-2 months. In the fall we found out that we would become uncles/aunts. Meanwhile, autumn passed, we planned, and still no pregnancy occurred. After New Year 2021, I decided to take hormones, and sent my husband to take SG. Everything is fine with him, mobility is 73%, of which 67 are fast, my progesterone is low and extradiol is 2 times increased. Both in phase 1 and phase 2. I only thought of going for an ultrasound on February 24, 2021. The diagnosis was simply a shock, endometrioid cyst 4*5 cm, the uterus is displaced to the left (it looks like adhesions). I went straight to the paid center, I didn’t dare look for the reason in our residential complex, the reviews were very disgusting. The gynecologist didn’t give me much reassurance, she looked at the tests and said that the chances with this formation and hormone levels are very small, but there are. We need to cut faster. She immediately suggested taking a few swabs, “they’ll still be useful during the operation.” Just have it cut in a normal clinic, so that you have something to plan for later. This happened at about 9DC, the DF was about 14mm. I still recommended looking at folliculometry in this cycle. I left the clinic with round eyes, told my husband, my husband said: “Go to another doctor!” By that time, I was already keeping the 4th BT chart, they were 2-phase, in the 2nd phase it was not above 36.9, but the temperature dropped 4 days before the start of menstruation. That's when the little mess began. In short, after the temperature rose, I went to see what was on the ultrasound. Ultrasound shows no ovulation, no VT, no fluid. But there is the same cyst and another doctor yelled at me with good obscenities that I had come to an ultrasound instead of a hospital. In short, after taking a pack of tests and ultrasound results, I entered our residential complex. She silently put everything on the doctor’s table, and although she was old, she seemed to be of sound mind. She immediately said, “Yes, it’s for surgery, we’ll give you a referral right now.” And a sheet for tests. True, we are now signing up almost a month in advance for tests.” I refused the free line for blood work and collected all the tests myself within 10 days, fortunately my medical relatives helped with this. I also decided to go to MONIIAG to find out what was going on with the operations and what the doctor would say in general. In MONIIAG there are queues for six months according to the quota, reasonable prices according to the contract, in the corridors there are a horror of people and a lot of “insiders”. At MONIIAG there is a 3-week queue for a paid appointment, if the queue moves, they called and invited you on an unpredictable day. As a result, 1 time I didn’t get to time, and the second time I got into an accident. I only got to the MONIIAG doctor on the 3rd attempt. As a result, I underwent surgery in Zhelezka in a new obstetric diagnostic center. The operation took place on March 31, 2017 under a quota. I arrived with a pack of tests and ultrasound results, head. The department looked at my list, estimated my DC and said that we have time to undergo surgery right in this cycle. They admitted me a week later and operated on the next day. According to the result: the tubes are passable, a huge 4*5 endocyst is in the lymph node, the entire left side is soldered to the intestines (together with the tubes, ovary and uterus). The operation lasted almost 3 hours. Apart from the cyst, there is no endometriosis. I jumped the next day to the delight of the nurses. After the operation, a new cycle began on April 12, 2021. Then I was put on 3 Zoladex injections. I stayed in the correctional colony for exactly 3 months + 2 weeks. July 17 - 42 days after the 3rd injection. I decided it was time for my first ultrasound. The result is a linear endometrium, small follicles on both sides, LN (operated) less than 2 cm in length, single follicles. They said there was no hope for him yet. Zoladex stopped frying. July 31 - abdominal pull, ultrasound, DF 18*19mm in the PU, endometrium 7mm. They sent me home to try harder. That “tomorrow” the follicle will most likely rupture. My husband was stunned, he said, I can’t do it under pressure. But everything worked out. August 01 - Ultrasound, DF did not burst, Ovitrel injection on the same day. It is rotten and there are no analogues anywhere in the region, because... not available from suppliers. YaB went. No one was in a fighting mood. August 02 – we tried again. They also laughed that we needed to work off the injection. August 04 - the pulling stopped, I had been sick all week, among the “snot” I found bright yellow stripes. Obviously, the follicle burst. August 05 - Ultrasound. The corpus luteum on the right is 18*19mm, the endometrium is 10mm. They prescribed angiovitis and progesterone 1*200. I didn’t drink either one, I just kept the 1 mg folk. I don’t know why there is such an overkill in the concentration of vitamins. Ovulation was set for August 4th. August 10 - ghost test. I didn’t get my hopes up, because... was ovitrel. But my stomach was pulling. like you're about to get your period. Herring and red fish were used. I’m ready to burst into tears over everything, I’m offended by every nonsense. August 11 is a ghost. According to the schedule, I already understood that it was IZ, but I decided not to twitch yet. August 14 - weak streak. Analysis for hCG and progesterone. Result: hCG 127, progesterone 100 nmol/l It turns out that I did not come out of menopause. See the doctor on Saturday. I'm really scared.