WhatDiseases > Women's diseases > Amenorrhea > Is it possible to get pregnant with amenorrhea?
Every woman at some point in her life asks the question, is it possible to get pregnant with amenorrhea? Before answering the question, you should establish the reason for the absence of the menstrual cycle, exclude concomitant pathologies and clarify what medications the patient is taking.
Is it possible to get pregnant with amenorrhea?
Causes of secondary amenorrhea
Only a specialist can determine the nature of the pathology after a comprehensive and thorough examination.
Among women
The factors that caused the absence of menstruation determine the severity of the pathology and the nature of its course. Thus, the functional causes of secondary amenorrhea are quite easily eliminated, but in more serious cases, when organic damage to the brain, uterus or ovaries is detected, treatment takes a very long time, and the prognosis is not always favorable.
Endocrine diseases
One of the main causes of secondary amenorrhea is a disruption in the production of hormones by the pituitary gland and hypothalamus, which may be due to the following factors:
- neoplasm of any etiology in the brain area;
- abnormalities of the blood vessels of the head;
- hematomas caused by head injuries or resulting from rupture of blood vessels;
- side effects from certain medications or their overdose;
- nervous exhaustion, increased stress;
- anorexia resulting from a nervous disorder.
Other disorders of the endocrine system that can cause secondary amenorrhea in medicine include:
- diseases of the thyroid gland, for example hypothyroidism - decreased levels of hormone production;
- excessive amounts in the body of hormones produced by the adrenal cortex (Itsenko-Cushing syndrome);
- hypocorticism (Addison's disease) - in this case, the adrenal cortex produces a small amount of the hormone cortisol, as a result of which the normal functioning of various organs is disrupted.
All of these diseases affect the functioning of the ovaries; they stop producing female sex hormones, causing hypogonadism.
The most common cause of secondary amenorrhea caused by disorders of the endocrine system is an increase in the concentration of the hormone prolactin in the female body - hyperprolactinemia. High levels lead to a complete imbalance of sex hormones.
We recommend reading about ureaplasmosis in women. You will learn about the causative agents of the disease and routes of transmission, manifestations of ureaplasmosis, drugs and treatment regimens.
And here is more information about hidden sexually transmitted infections.
Tumors in the pituitary gland and hypothalamus
Secondary amenorrhea can be caused by neoplasms of any etiology, but in clinical practice, malignant tumors in this area of the brain are quite rare.
Early menopause
Premature menopause is considered to occur when a woman has not reached the age of forty. The reason for premature cessation of menstruation may be:
- ovarian depletion, i.e. a condition when the synthesis of female sex hormones and the maturation of follicles stop;
- autoimmune pathologies, when the body begins to produce antibodies that suppress its own cells (resistant ovarian syndrome);
- previous surgery to remove the ovaries or trauma to them;
- genetic predisposition;
- bad habits, especially smoking;
- treatment of oncological diseases using radiation therapy and chemotherapy.
Physiological menopause
This is a natural state of the female body, when at the age of 45 - 55 years the ovaries cease to perform their function, the egg is no longer produced.
Weight loss
The fashion for extreme weight loss, according to doctors, has led to a sharp increase in the number of cases of secondary amenorrhea. Currently, more than 25% of this pathology occurs due to a sharp decrease in body weight. Low-calorie diets, complete abstinence from carbohydrates and excessive protein consumption in a short time can lead to the loss of 15% of adipose tissue, without which female sex hormones cannot be produced.
If a woman is diagnosed with anorexia, this almost always indicates a decline in ovarian function.
Stress
Secondary amenorrhea, caused by excessive emotional stress, is typical mainly for young girls. They are more likely than adult women to experience a state of distress when the body cannot cope with emotional overload.
Such a shock can lead to a sharp decrease in body weight, weakened immunity, and disruption of the endocrine system. As a result of such a load on the body, the pituitary gland reduces the synthesis of gonadotropic hormones, and menstruation stops.
Damage to the uterine lining
Such injury can occur as a result of instrumental intervention, most often during the process of artificial termination of pregnancy. In some cases, curettage is required after childbirth, when polyps form on the uterine lining or when there is heavy bleeding.
Polycystic ovary syndrome
In addition to complaints about the absence of menstruation, women with this disease suffer from excess male-pattern hair growth on the face and body. This is caused by excessive production of male sex hormones by the female body. Most often, girls of reproductive age suffer from this disease. Also, among patients with this diagnosis, there are a lot of severe obesity and diabetes mellitus.
In teenagers
The causes of secondary amenorrhea in girls under 15 years of age are generally the same as in adult women. The absence of menstruation may be due to the fact that their body image is disturbed, which provokes changes in eating behavior. Girls begin to lose weight intensively, leading themselves to anorexia nervosa or, conversely, “eating” stress, which leads to bulimia or obesity. Sometimes, against the background of such disorders, a teenager may develop psychosis.
Also at this age, secondary amenorrhea can be caused by increased physical activity during sports or strong emotional experiences.
Amenorrhea during pregnancy
Pregnancy with amenorrhea is a physiological condition when the processes of egg maturation in a woman’s body temporarily stop. This feature is due to powerful hormonal changes and a change in the background of estrogen activity. Follicle-stimulating and luteinizing hormones cease to be produced, and ovulation stops. This is necessary to prevent desquamation of the endometrium with the attached fertilized egg, in order to prevent spontaneous abortion.
What you need to know about lactational amenorrhea During the entire period of pregnancy, ovulation does not occur, eggs do not enter the fallopian tubes for maturation, and mucociliary clearance reduces its activity. The listed changes are physiological, so it is impossible to become pregnant again. Perinatal amenorrhea lasts until the end of pregnancy. At the time of childbirth, the hormonal balance is rearranged, after a massive release of oxytocin, required for normal labor, the synthesis of prolactin begins. Prolactin leads to the development of lactational amenorrhea.
Types and their features
The types of secondary amenorrhea are determined by the disease that caused the cessation of menstruation.
Uterine form
This form of secondary amenorrhea occurs due to the formation of adhesions in the uterine cavity. Over time, the uterus begins to become deformed, and then can become completely overgrown. Adhesions are formed as a result of injury to the endometrium; the mucous membrane at the site of injury begins to be replaced by formations of connective tissue, which gradually grow together.
The endometrium is most often injured during instrumental intervention during abortion, surgery to remove fibroids and polyps, cesarean section or diagnostic curettage.
Often, adhesions are formed as a result of inflammation caused by an infection that has entered the uterine cavity, if the woman did not consult a doctor in time and did not undergo a full course of antibacterial therapy.
Diagnostic curettage, removal of polyps and fibroids in the uterine cavity are common causes of adhesions and the development of secondary amenorrhea
Sometimes adhesions can be caused by an intrauterine device if it is not installed correctly or is rarely changed.
Iatrogenic form
Secondary amenorrhea of this type occurs as a result of treatment of any organ disease, for example, division of a bicornuate uterus or surgery to remove fibroids.
Central genesis
Pathology occurs due to a violation of either the function of subcortical structures or the cerebral cortex.
Secondary amenorrhea of this type occurs as a result of the negative impact of environmental factors, for example, severe stress or nervous strain.
Most often, the moment of cessation of menstruation is preceded by intoxication of the body, mental trauma, pregnancy with complications, or neuroinfection. Amenorrhea of central origin is found in 30% of women suffering from schizophrenia and other mental illnesses.
Lactation
It is not a pathology. There is no menstruation after childbirth during full breastfeeding. This is due to the fact that the lactation process leads to a constantly increased level in the blood of the hormone prolactin, the function of which is to produce a portion of milk after each feeding. Increased concentrations of prolactin suppress gonadotropic hormones of the pituitary gland.
About lactational amenorrhea, watch this video:
Causes of primary amenorrhea in adolescents
Complaints about the absence of menstruation during puberty are not a frequent reason to consult a gynecologist, although they can be a manifestation of serious diseases. The causes of primary amenorrhea are divided into three main groups:
- the absence of menstruation is caused by the anatomical features of a teenager;
- the pathology is caused by hereditary factors;
- problems with the menstrual cycle were the result of emotional and psychological disorders.
Classification of amenorrhea
Anatomical causes of primary amenorrhea often arise in the prenatal period, when the girl’s genitals begin to form.
In some cases, during the first gynecological examination, a teenager is found to have a too narrow or completely closed entrance to the vagina. Such anatomical features do not allow menstrual blood to escape, so it accumulates in the uterine cavity, which is fraught with the occurrence and development of inflammatory processes in the organs of the genitourinary system. Also, such a development of pathology can cause inflammation of the peritoneum and other dangerous consequences.
Primary anatomical amenorrhea is usually characteristic of girls with underweight and underdeveloped secondary sexual characteristics. To make an accurate diagnosis, it is necessary to do an ultrasound of the pelvic organs.
Genetic causes of primary amenorrhea are also often identified during the first visit to the gynecologist. Sometimes, when collecting anamnesis, it turns out that in the teenager’s family there are the same deviations in close relatives, for example, the mother or older sister had a late onset of menstruation.
Genetic anomalies in amenorrhea are associated with damage or inferiority in the 23rd pair of X chromosomes, which are responsible for the functioning of the ovaries.
In recent years, gynecologists are increasingly faced with cases in which adolescents complaining of lack of menstruation have neither hereditary nor anatomical factors for the occurrence of amenorrhea.
When examined, about a third of all girls with menstrual irregularities are diagnosed with psycho-emotional problems, constant stress, excessive physical activity, for example, playing professional sports, anorexia, and excessively strict diets for weight loss. For many of them, the cycle is restored over time without medical intervention, but sometimes qualified medical assistance is required.
This form of amenorrhea is called “central” and is caused by problems in the hypothalamus, one of whose functions is to control menstrual function. In rare cases, a brain tumor may be a factor in the development of central amenorrhea.
In general, the causes of primary amenorrhea can be formulated as follows:
- abnormalities in the development of the uterus and gonads (gonadal dysgenia);
- genetic pathology in which girls have one X chromosome missing or damaged (Shereshevsky-Turner syndrome);
- lack of sensitivity of tissues to male sex hormones, when the set of chromosomes in girls corresponds to male (textile feminization syndrome);
- problems with the hypothalamus;
- pathologies of intrauterine development that caused vaginal fusion;
- anorexia, improper diet;
- excessive physical activity;
- constant stress, nervous tension.
A thorough comprehensive examination of the teenager will allow you to determine the cause of primary amenorrhea.
We recommend reading about the treatment of algodismenorrhea. You will learn about the causes of primary and secondary algodismenorrhea, symptoms in adolescents and adult women, treatment options.
And here is more information about ovarian dysfunction.
Is it possible to get pregnant with secondary amenorrhea?
This question does not have a clear answer, since the possibility of conception depends on the type of pathology. For example, amenorrhea caused by eating disorders, stress, and heavy physical activity has a good prognosis. In this case, normalization of lifestyle and adequate treatment can quickly improve the general condition of the body systems and establish a normal menstrual cycle.
The following types of secondary amenorrhea can be corrected and make it possible to become pregnant and give birth to a child:
- central genesis - after a course of hormonal therapy, despite the complexity of treatment, in 95% of cases it is possible to achieve the onset of menstruation and achieve the desired result;
- with uterine pathology, pregnancy is possible after removal of adhesions through surgery.
A much less optimistic prognosis for possible pregnancy with secondary amenorrhea caused by polycystic ovary syndrome. According to medical statistics, only 20% of women with this diagnosis have the opportunity to give birth to a child. But modern methods of diagnosis and treatment of this disease can increase the chances of success with timely consultation with a doctor and adequate treatment.
If follicles are found in polycystic disease at least in minimal quantities, a woman has a chance of becoming pregnant after drug stimulation of ovulation or, in case of failure, using a donor egg.
Amenorrhea during lactation
Pregnancy after amenorrhea occurs at the end of breastfeeding, when the baby is less likely to latch onto the breast. As a rule, this occurs by the sixth or eighth month of the baby’s life as a result of the introduction of the first complementary foods, replacing one or two daily feedings. A period such as lactation is extremely important for every woman, for:
- maintaining her health;
- activation of the mammary glands;
- recovery after childbirth;
- healthy nutrition for baby.
Breastfeeding in the first week after birth stimulates active contractions of the uterus and its return to its previous size. It is impossible to get pregnant in the first months of active breastfeeding at intervals of no more than three hours. This is due to increased prolactin activity, contraction of the uterus and a complete absence of ovulation. The endometrium does not undergo desquamation and gradually grows in anticipation of the first menstrual cycle. To maintain amenorrhea longer, World Health Organization breastfeeding experts recommend extending nighttime co-sleeping with your baby and maintaining night feedings for up to two years.
In the first six months of lactation, a woman may experience problems with milk production. This requires plenty of fractional drinking, meat food and a good night's rest. To improve the process of breastfeeding, which is extremely important for every child, a woman can turn to specialists for help. At this time, contraception using the lactational amenorrhea method is the most effective and safe. Pregnancy does not occur until the first break between feedings is more than three hours in 83% of women due to egg immaturity.
As the child grows and develops, there is a gradual involution of the glandular tissue of the mammary gland, degeneration of the milk ducts and a decrease in the intensity of milk production. Prolactin is synthesized in response to the baby being put to the breast; infrequent feedings return the menstrual cycle. During this period, the normal maturation of the egg is sharply restored, and the hormonal background becomes the same as before pregnancy. You can get pregnant in the first menstruation after childbirth, even if your cycle is irregular or without heavy bleeding.
Body examination
The first stage of diagnosis is the mandatory collection of anamnesis to determine the signs of pathologies that caused the cessation of menstruation. During the initial examination, the doctor must establish the history of menstruation, the nature of sexual activity, and the contraceptives used. It is also necessary to obtain information about existing hereditary diseases and infections suffered in childhood.
Next, the doctor conducts a gynecological examination, but it is not informative, except in cases of tumors in the appendages or inflammatory processes of the genitourinary system.
Laboratory tests are required:
- blood serum test for hCG to exclude pregnancy;
- determination of prolactin concentration in blood plasma to exclude pituitary tumors;
- determination of the ratio of luteinizing (LH) and follicle-stimulating (FSH) hormones;
- karyotype study to exclude the Y chromosome;
- performing a glucose sensitivity test;
- carrying out a progesterone test.
If laboratory tests were not informative enough to determine the causes of the pathology, special studies are prescribed:
- if polycystic ovary syndrome is suspected, laparoscopy is necessary to determine the degree of patency of the ducts and ovaries;
- To determine the presence of a cyst or fibroids in the uterus, ultrasound diagnostics are performed;
- determination of endometrial functionality;
- computed tomography and MRI to diagnose brain disorders.
Based on the results of the study, the doctor can determine the cause of secondary amenorrhea and prescribe the correct treatment.
For information on basic examinations for menstrual irregularities, watch this video:
Diagnostics
It is almost impossible to independently determine why violations occurred.
The causes of amenorrhea in adolescents are often rooted in genetic developmental disorders and abnormalities of the genital organs.
Therefore, only a specialist can finally figure out the problem after a thorough examination of the girl. The research package most often includes the following:
- Standard examination with determination of weight, height, constitution, presence of secondary sexual characteristics, etc.
- Ultrasound examination of the pelvic organs, which can detect abnormalities in the structure of the internal genital organs.
- Functional study with determination of the level of various hormones in the blood. It is mandatory to determine LH, FSH, testosterone, estradiol, cortisol (produced in the adrenal glands), progesterone, DHEA, prolactin, T3 and T4 (synthesized in the thyroid gland) and some others at the discretion of the pediatric gynecologist or endocrinologist.
- After complex examinations, various tests with hormones can be carried out to check whether the body responds to them or is intact.
- In the future, in most cases, it is necessary to perform an X-ray of the skull, CT or MRI of the brain if a microadenoma of the pituitary gland or pathology of the sella turcica is suspected.
- Fundus examination may suggest certain genetic disorders and brain tumors.
- It is also necessary to determine the girl’s karyotype to exclude chromosomal pathologies.
The scope of the examination can be expanded depending on the basic test results at the discretion of the attending physician.
We recommend reading the article about ways to call your period. From it you will learn about whether it is necessary to induce menstruation and whether this can be done, effective medications for delay, and the use of folk remedies.
Treatment of secondary amenorrhea
Treatment methods depend on the factors that caused the cessation of menstruation.
If the absence of menstruation is associated with anorexia, the woman is prescribed a diet high in protein. To eliminate disorders of the nervous system, sedatives and a course of psychotherapy are indicated.
With obesity, on the contrary, it is important to switch to a low-calorie diet and a proper work and rest schedule.
If, as a result of the examination, resistant ovarian syndrome is diagnosed, stimulation of ovulation using the drug Clomiphene is indicated. The course of treatment lasts 1 - 3 months and ends after the menstrual cycle normalizes.
If tumors are detected in the ovaries or pituitary gland, surgical intervention is indicated.
For diseases of the thyroid gland, long courses of thyroid-stimulating hormones are prescribed.
Any course of hormonal therapy can only be prescribed by an endocrinologist. To achieve results, its recommendations must be strictly followed.
Classification
Due to the diversity of causes and pathogenetic mechanisms for the development of primary amenorrhea, in modern science there are no uniform principles for systematizing the forms of pathology.
According to the most commonly used classification, primary amenorrhea is distinguished:
- with delayed sexual development, when girls begin to develop secondary sexual characteristics too late, or they are poorly developed;
- without delayed sexual development, when secondary sexual characteristics develop normally and in a timely manner, but there is no menstruation.
With type 1 amenorrhea, girls aged 16 years and older are completely absent of menstruation, while they do not experience enlargement of the mammary glands, the appearance of hair in the pubic and axillary area, weight and height indicators that lag behind the average for this age group, and a discrepancy between the degree of bone ossification and the calendar number of years.
In the absence of menstruation against the background of normal puberty, pathologies of the development of the genital organs are most often found - the complete absence of the natural exit from the vagina or hymen (gynathresia), or significant underdevelopment or complete absence of the uterus (aplasia).
A more expanded classification is based on identifying the level of pathology:
- the level of the hypothalamus and pituitary gland, this form occurs in 12% of cases, most often caused by infectious diseases suffered in early childhood, birth trauma, neoplasms in the area of the pituitary gland and hypothalamus, nervous and physical overload;
- ovarian level, when a girl’s pathology develops even before birth due to improper development of chromosomes;
- the level of the uterus and vagina, when due to anatomical features the outflow of menstrual blood becomes impossible, this type of pathology is called false amenorrhea;
- hormone levels, when the absence of menstruation is associated with disturbances in the production of corticosteroids.
Causes of amenorrhea depending on the level of damage to the reproductive system.
Reliable diagnosis of the form of the disease and the causes that caused it is the key to successful therapy.
Treatment
The disease is treated by an endocrinologist-gynecologist or gynecologist with mandatory consultation with an endocrinologist.
When detecting abnormalities in the pituitary-hypothalamic system and delayed sexual development, a test with an analogue of gonadotropin-releasing hormone (GnRH) is used. If a girl’s body has a positive response to a test with a GnRH analogue, then treatment can be non-hormonal. They begin with the use of neurotropic and vitamin complexes in order to improve the connection between the cerebral cortex, the structures of the hypothalamus and pituitary gland. In some cases (especially if the cause of amenorrhea is nervous disorders) this has an effect. If there is no reaction to a test with a GnRH analogue, hormonal drugs are immediately prescribed for replacement purposes.
If a pituitary tumor is detected, it is removed. With the introduction of external hormones, a girl will catch up with her peers in development and the menstrual cycle will improve. The prognosis for childbearing is favorable; IVF may be used.
If genetic chromosomal abnormalities are determined and there are no ovaries in the girl’s body (gonadal dysgenesis), it is necessary to immediately begin hormone replacement therapy so that the girl develops externally in accordance with her age. If there is an extra Y chromosome in the girl’s chromosome set, then before starting HRT it is necessary to remove the connective tissue cords that replace the ovaries. This is done in order to prevent the growth of malignant tumors from connective tissue cords, which often develops with such a chromosome set.
In case of genetic chromosomal abnormalities and the absence of normal ovaries in a girl, hormone replacement therapy is indicated for a long time, until the age of middle menopause. Of course, the girl herself will not be able to conceive and give birth.
Vaginal malformations are successfully operated on. Girls menstruate, are sexually active and conceive a child after plastic surgery. If the hymen is closed and there is a septum in the vagina, they are dissected.
Plastic surgery to create an artificial vagina in the absence of one requires hospitalization in central clinics and highly qualified operating gynecologist.
In the absence of a uterus (Rokitansky-Küstner syndrome), plastic surgery to lengthen the vagina is sometimes also necessary for a full sexual life. In this situation, the ovaries work in accordance with age; hormone replacement therapy is not indicated. Plastic surgery to create an artificial uterus is not currently used. If a woman wishes to have a child, her egg is fertilized using IVF, and the pregnancy is carried to term by a surrogate mother.
Symptoms of pathology
The main difference between amenorrhea and other female diseases is the absence of menstruation for six months or more, but against this background, signs of the pathologies that were the cause of the development of this phenomenon always appear:
- If primary amenorrhea is caused by anatomical problems, then blood accumulates in the uterus, which causes severe cramping pain in the lower abdomen. These pains appear cyclically on the days when menstruation should begin, and last on average 2 to 3 days. Associated symptoms are headache, nausea, enlarged mammary glands and increased sensitivity.
- If the absence of menstruation is associated with neoplasms in the pituitary gland, girls experience increased irritability, an unstable emotional state, mood swings, headaches and other psycho-emotional disorders.
- With primary amenorrhea of a genetic nature, underdevelopment of the genital organs is detected in girls of puberty. Often teenagers differ from their peers by being too tall, having long limbs with a fairly short body.
Shereshevsky-Turner syndrome
- If the pathology is caused by disturbances in the functioning of the ovaries, its symptoms may include excess weight, acne, too noticeable hair on the body and face, and increased levels of insulin in the blood. This form of primary amenorrhea is fraught with the development of osteoporosis.
The complex of identified symptoms of primary amenorrhea allows the doctor to determine treatment tactics depending on the nature of the disease that caused this pathology.
For information about the causes of primary amenorrhea, watch this video:
Treatment and clinical recommendations for primary amenorrhea
Knowing the classification and what it is, let’s try to figure out how to cure primary amenorrhea. Today, treatment of primary amenorrhea is carried out in accordance with modern clinical recommendations of Russian and European associations of endocrinologists.
Treatment of primary amenorrhea with gonadal dysgenesis depends on the presence or absence of the Y chromosome in the teenager’s karyotype, since its presence increases the risk of malignancy and requires surgical removal of such gonads as early as possible. If it or the gonads have already been removed, then HRT is indicated for a long time, containing natural hormones and not containing androgenic effects.
Dysfunction of the hypothalamic-pituitary system in the constitutional form does not require treatment, but organic lesions require hormone replacement therapy, which is necessary for the development of sexual characteristics and the appearance of menstruation, which have a positive effect on the mental health of a woman.
Primary amenorrhea: treatment for developmental defects such as uterine aplasia (Mayer-Rokitansky-Küstner syndrome) is only surgical. Its essence lies in colpoiesis from the peritoneum of the pelvic part through the vagina in combination with laparoscopy. The next stage is plastic restoration of the vagina, which allows sexual activity. If ovarian function is preserved, then hormonal treatment is not indicated. Often, against the background of uterine aplasia, functional ovarian cysts appear, which requires careful monitoring of them using ultrasound, and when they are identified, antigonadotropic therapy is indicated to promote their regression. In such cases, pregnancy is impossible, and only surrogacy is the only method of assisted reproductive technologies for the birth of a genetically own child.
To treat both types of amenorrhea, hormone replacement therapy is prescribed in order to activate the work of the ovaries. If primary amenorrhea occurs due to anomalies of physical development, then therapy can be prescribed for life.
In case of any anatomical reasons, treatment occurs through surgery.
Young girls should not get carried away with diets, so as not to slow down sexual development.
The main symptoms of amenorrhea are the absence of the onset of the menstrual cycle, as a result of which reproductive functions are impaired, which leads to infertility. The ovaries are unable to produce hormones to maintain a normal cycle. In most cases, the causes of amenorrhea can be eliminated and the menstrual cycle can be normalized.
Infertility that cannot be treated can be a complication of amenorrhea. In this case, IVF, insemination with partner's sperm or ovulation induction can help.
In order to exclude amenorrhea, you must:
- Visit your gynecologist regularly. A timely visit to the doctor will help prevent complications such as infertility
- maintain a healthy lifestyle
- have a regular sex life.
Treatment begins with the use of estrogens. The dosage is selected individually by the doctor. After 12 months of treatment, an additional hormone progesterone is administered, gradually increasing the dose of estrogen. This tactic helps to achieve puberty in a child within a couple of years.
If the patient is taking growth hormones, estrogen may be prescribed before age 15. Otherwise, a deferment is made, but no later than this age.
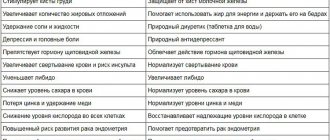
The effect of hormonal therapy:
- Helps in the development of a girl’s breasts, affects the maturity of the uterus and appendages.
- Positive dynamics of pubic hair growth and in the armpit area.
- Decreased concentration of gonadotropins.
- Maturation of eggs and the appearance of the menstrual cycle.
- Prevention of heart and skeletal diseases.
- Adaptation in society.
- Improving the quality of life.
When a patient desires to have a child, artificial insemination (IVF) surgery can come to the rescue. This procedure increases the chances of becoming a mother, but also has serious risks. Since most patients diagnosed with primary amenorrhea have disturbances in the functioning of the circulatory system, including the heart, during childbirth there is a risk of aortic rupture in 2% of women, and the fatal outcome of such childbirth is 100 times more likely. Therefore, in the presence of these anomalies, the IVF procedure may also be contraindicated. The decision for each patient is made separately by the attending physician.
In conclusion, I would like to note that such a disease as primary amenorrhea can be false, and menstruation comes, but a little later. The development of primary true amenorrhea is very rare, and the diagnosis of gonadal dysgenesis is even rarer.
But if you have this disease, you still shouldn’t be upset. It responds well to treatment, and the girl’s chances of becoming a mother increase significantly.
Therefore, the question of primary amenorrhea and pregnancy is quite individual. Which we'll talk about below.
Methods for diagnosing amenorrhea
Gonadal dysgenesis is the most common cause of the development of primary amenorrhea with delayed development of secondary sexual characteristics. Occurs in 30-40% of cases. This diagnosis is characterized by the absence of functional hormone-producing tissue.
Doctors distinguish several forms of primary amenorrhea:
- Typical.
- Erased.
- Mixed.
- Clean.
When examining the patient, one can see such developmental defects as genital infantilism, underdevelopment of the mammary glands, atrophy of the vaginal and vulvar mucosa. In the future, to specify the diagnosis of primary amenorrhea, it is necessary to conduct an examination.
In gynecology, primary amenorrhea is a serious female disease. It is characterized by the complete absence of menstruation throughout life, starting from puberty. It is extremely rare and accounts for 10% of the total number of amenorrheas encountered. Among women of reproductive age, the incidence of the disease is 1.5-3%.
Signs that may indicate illness
When examining a girl, a doctor should be alert to the following signs:
- Lack of menstruation after age 16.
- Inhibited appearance of secondary sexual characteristics (underdevelopment of the mammary glands, lack of hair).
- Absence of menstruation after the development of sexual characteristics for several years.
- Imbalance of weight and height, disharmonious development.
These factors can be noticeable to the parent's eye, and any deviation from the norm should not be ignored.
Diagnosis of gonadal dysgenesis
The most revealing tests for diagnosing the disease are blood tests for hormones. A sharp increase in gonadotropins and a decrease in the hormone estradiol against their background will be indicative.
An analysis for a hormonal test with gestagens may also be offered. A negative answer indicates a problem with the ovaries and excludes uterine amenorrhea.
Differential diagnosis will be prescribed for violations of the development of sexual characteristics.
Thus, the disease will be indicated by:
- Primary amenorrhea.
- Underdevelopment of secondary sexual characteristics.
- Increased FSH.
- Incorrect set of chromosomes in the karyotype, lack of sex chromatin.
- Negative histogen test.
- Positive estrogen test.
If the Y chromosome is present in the karyotype, the gonads are surgically removed using the endoscopic method. The procedure is recommended for people under 20 years of age. In the absence of this chromosome, only hormone replacement therapy is carried out.
Causes
We know the international classification of primary amenorrhea, now it remains to find out what is the cause of primary amenorrhea.
Primary amenorrhea: its causes can be genetic, anatomical or psycho-emotional.
Among hereditary causes, the main place belongs to diseases transmitted genetically and characterized by abnormal sex chromosomes.
The anatomical cause of primary amenorrhea is a delay in the physical development of a certain physique - a thin, low-weight woman with undeveloped or poorly developed mammary glands, a narrow pelvis, lack of female hair growth, as well as disturbances in the development of the reproductive organs. Primary amenorrhea - the reasons for its appearance are most often due to:
- underdevelopment of the sex gonads, i.e. dysgenesis
- hereditary Shereshevsky-Turner syndrome, where the X chromosome, responsible for the sexual development of a girl, is missing
- hypopituitarism
- congenital malformations of the reproductive organs that formed at the stage of their formation or exposure to unfavorable factors during this period. This can be either underdevelopment of an organ or its absence
- tumor formations of the central nervous system
- strong impact of stress, worries and psycho-emotional experiences
- poor nutrition and various diets
- significant physical activity during embryogenesis.
- testicular feminization syndrome, in which the tissues are not sensitive to androgens and then boys are born according to the genotype, and according to the phenotype, girls are born with underdeveloped testicles in the abdominal cavity.
So, primary amenorrhea occurs as a result of chromosomal aberrations, dysfunction of the brain as a result of exposure to a severe stressful situation, increased physical activity during puberty, severe stress and starvation, as well as as a result of the impact of a tumor process in the brain. An important role in the development of primary amenorrhea is assigned to the pituitary gland, since if its work malfunctions, the production of all hormones in the body is disrupted.
The easiest thing to diagnose during an examination is to determine the incorrect development of the reproductive organs, such as overgrowth or narrowing of the vagina, uterus or its part - the cervix, which leads to the accumulation and retention of blood in the cavities, while causing pain and inflammation, leading to the development of many complications.
There are several factors influencing the dysfunction of a girl’s reproductive system:
- Gonadal dysgenesis (occurs in most cases).
- Müllerian agenesis (such patients have a congenital absence of a vagina or uterus).
- Hypothalamic disorders.
- Delayed puberty.
- Excessive physical activity, violation of daily routine and nutrition.
- Anatomical features of a woman.
- Congenital resistance to gonadotropins.
These are the most common situations that affect the absence of menstruation in a girl of reproductive age. Each problem requires an individual approach and treatment under the supervision of an experienced doctor. Primary amenorrhea is characteristic of Mayer–Rokitansky–Küstner syndrome.